What is Golfer`s elbow?
Golfer`s elbow (GE) is tendinopathy caused by overuse or overload and affects the medial common flexor tendon of the elbow. It is medically known as “medial epicondylitis” and also commonly referred as “pitcher`s elbow” or “baseball elbow”. This may present insidiously with patients reporting with an aching pain that radiates from the epicondyle down to the wrist. (https://www.ncbi.nlm.nih.gov/books/NBK519000/)
Who are at risk of getting GE?
Less than 1% population has GE. It affects men and women between ages 45-64 years. Women are slightly more likely to develop GE than men. Approximately 90% of people with GE develop the condition doing something other than playing sports. It usually affects the dominant arm and symptoms appear on the inner aspect of the elbow around the bony prominence. (https://my.clevelandclinic.org/health/diseases/21711-golfers-elbow-medial-epicondylitis)
Risk factors in athletes include training errors, improper technique, equipment or functional risk factors including lack of strength, endurance or flexibility. Occupation related risk factors include heavy physical work, excessive repetition, high body mass index, smoking, high psychosocial work demands. General risk factors include type 2 diabetes and tobacco use. In women, obesity is associated with increased risk. (https://www.ncbi.nlm.nih.gov/books/NBK519000/)
What are the causes of Golfer`s elbow?
GE is caused by the excessive force used to bend the wrist towards the palm. This can happen while:
What is the pathophysiology of GE?
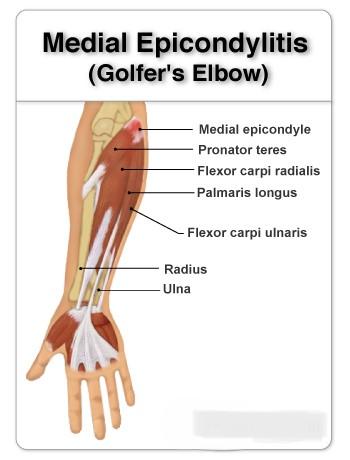
Medial epicondylitis is overuse tendinopathy due to chronic repetitive concentric or eccentric loading of wrist flexors and pronator teres resulting in angiofibroblastic changes. Repetitive activity leads to recurrent microtears within the tendon and subsequent tendinosis. Literature suggests all flexor muscles are affected equally except palmaris longus. There is no evidence of bony inflammation. As the tendon undergoes repetitive microtears, there is remodeling of the collagen fibers and increased mucoid ground substance. Focal necrosis or calcification can occur.
Subsequently, collagen strength decreases leading to increased fragility, scar tissue formation and thickening of the tendon. Rarely, acute trauma can also cause golfer`s elbow from sudden violent contraction of the flexor muscles.
What are the symptoms of GE?
Symptoms may take weeks or months to develop. They might start with pain in inner elbow that might seem worse in the morning. Other associated symptoms can be:
How is GE diagnosed?
Patient history will reveal sustained, prolonged, repetitive, overuse or traumatic episode of the affected extremity. The presenting symptoms will be medial elbow pain radiating into the forearm and wrist reported to be worse with forearm motion, gripping or throwing. Pain resolves with cessation of activity. Up to 20% of patients diagnosed with golfer`s elbow have ulnar nerve symptoms.
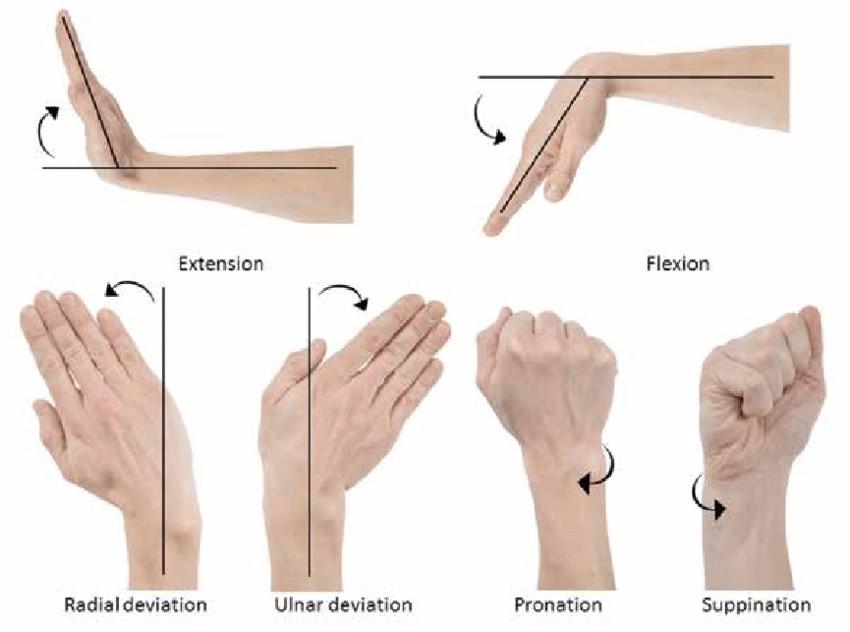
On examination there may be swelling, redness and warmth in acute cases. There maybe tenderness on palpation at 1 centimeter distal and anterior to the medial epicondyle. Resisted forearm pronation or wrist flexion elicits pain. In acute cases, passive wrist extension with extended elbow may reproduce pain. The range of motion at elbow and wrists are usually normal.
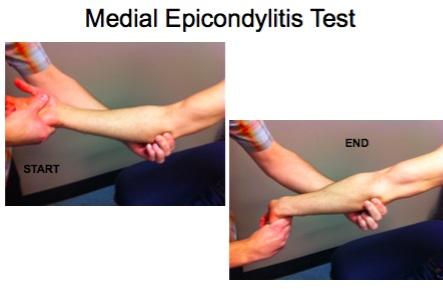
The GE test or medial epicondylitis test involves an active and passive component. In the active component, the patient resists wrist flexion with the arm in extension and supination. The passive component includes wrist extension with elbow extended. The test is positive if either or both maneuvers reproduce pain. Tinel`s test should be evaluated to assess ulnar neuropathy at the elbow. Ulnar collateral ligament integrity testing may be important in pitching sport athletes.
Imaging – GE is diagnosed largely based on clinical examination. X-rays are usually normal and maybe helpful in ruling out other possible diagnosis for e.g. periostitis, calcific tendinopathy.
Ultrasound and MRI can give clear indication of the diagnosis, and rule out other soft tissue or bone-related pathologies. Electromyography can be advised in case of ulnar neuropathy. (https://www.ncbi.nlm.nih.gov/books/NBK519000/)
What are the treatments for GE?
Treatment begins with avoiding the activity that causes pain.
Physical therapy is the primary modality of management for GE. The goal is to achieve full and pain free range of movements at the affected elbow. Modalities that may help with achieving goals include dry needling, extracorporeal shockwave therapy, electrical stimulation, iontophoresis, phonophoresis and therapeutic ultrasound. Soft tissue and joint manipulation techniques appear to allow more vigorous strengthening and stretching, resulting in better and faster recovery from the symptoms of GE.
Wearing a brace during the day while working or using night splints during sleep helps support the healing tendons. Kinesio taping for GE is also known to help reduce symptoms as it helps to off-load tendons.

Prognosis of golfer`s elbow is favorable. Most patients can return to work or sport after completing their physical therapy and activity modification. (https://www.ncbi.nlm.nih.gov/books/NBK519000/)
To get more personalized answers,
download now


Your trusted health companion, delivering personalized and precise answers in real-time, ensuring informed decisions for a healthier you