What are the treatments for PD?
There is currently no cure for Parkinson’s, but things like medication, surgical treatment, and lifestyle changes can provide effective symptom control for a long time. (https://parkinsonseurope.org/i-have-parkinsons/treatment/)
Medication for motor symptoms
Parkinson’s motor symptoms are caused by a lack of the chemical dopamine in the brain. Medication to treat these symptoms works in different ways to:
Motor symptom Parkinson’s medications include:
LEVODOPA
This is the most widely used Parkinson’s medication – it works as a chemical building block which your body then converts to dopamine in your brain. It can help greatly with stiffness and slowness of movement, as well as non-motor symptoms like swallowing and speech problems.
You’ll start with quite a low dosage of levodopa and build up gradually, and your doctor might experiment with different dosage levels and forms (controlled-release tablets, dispersible tablets or intestinal gel) to find the right balance for you.
One of the side-effects of levodopa is dyskinesia (involuntary body movements) which happens when the way your body absorbs and responds to the Levodopa changes over time. With disease progression, the Levodopa may not last as long in your system and therefore you may experience “off periods”. This is why it’s important to keep speaking to your doctor so they know you may need a different treatment regime.
COMT inhibitors
The symptoms of Parkinson’s are caused by a decrease in the levels of dopamine in the brain – so to reduce symptoms, you need to find ways to increase dopamine (like levodopa) or block/ “inhibit” any enzymes that break down dopamine in the brain, like Catechol-O-methyl transferase (COMT).
There are three main COMT inhibitors: entacapone, opicapone and tolcapone, although the latter is only used if the first two aren’t suitable, as it can cause liver damage. The levodopa drug Stalevo also contains COMT inhibitors.
Dopamine agonists
Prescribed both on their own or alongside other drugs like levodopa, dopamine agonists work by supporting the action of dopamine in the brain’s neuronal synapses.
Although not quite as effective as levodopa, they can provide good symptom control.
Dopamine agonists can be prescribed as tablets (including prolonged release ones), as a skin patch, pen injection or pump infusion. As well as helping to control movement issues, they also help with non-motor symptoms like sleep problems, pain and low mood.
MAO-B inhibitors
Monoamine Oxidase B, or MAO-B breaks down dopamine. MAO-B inhibitors help to maintain dopamine levels in the synapse for longer.
MAO-B inhibitors are either used on their own (usually in the beginning stages of Parkinson’s) or alongside other drugs like levodopa. They’re usually prescribed as tablets, but there’s also a version that dissolves on the tongue, and a liquid preparation for those who have swallowing issues.
Anticholinergics
In the brain, there is normally a balance between the activity of dopamine and the activity of acetylcholine, a neurotransmitter that helps to send messages from your nerves to your muscles.
But in Parkinson’s a deficiency in the brain of the neurotransmitter dopamine causes over-activity of acetylcholine. Anticholinergics work by blocking acetylcholine’s activity to restore this balance and help reduce your Parkinson’s symptoms.
These medications are older and are not used very often for Parkinson’s today. Sometimes they are prescribed for reducing tremor and muscle stiffness, either on their own (in the early stages of Parkinson’s) or alongside drugs like levodopa. They can also have positive effects on drooling issues.
Side-effects, such as memory impairment and other neuropsychiatric complications, limit their use, particularly in the elderly.
Non – motor symptom medications are the standard medicines given to treat symptoms such as dementia, anxiety, depression, sleep problems, etc. These medications are used for patients with or without PD.
If medications are unable to adequately control symptoms, the doctor may recommend surgery.
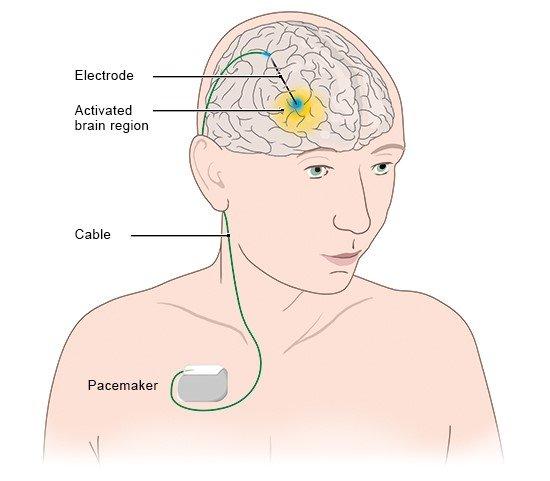
What is deep brain stimulation (DBS)?
DBS therapy uses a small, pacemaker-like device to send electronic signals to a precise area in the brain that controls movement via very thin wires. Stimulation of these areas appears to block the brain messages that cause disabling motor symptoms and so can provide greater symptom control.
A pre-operative MRI or CT is done to map the brain, followed by the surgical process of lead placement in the specific area of the brain. Neurostimulator implantation under the chest skin can be done on same day or few days later which will be connected to the leads using extensions that are placed under the skin from the chest, up to your neck and head.
Once you’re healed from surgery, a specialist will configure your programmer, adjusting it over several sessions to give a level of stimulation that provides the best possible symptom control. Depending on your device, you may have a controller that allows you to turn the system on and off, adjust the stimulation and check the battery.
What is the role of Neuroprotection?
In the context of Parkinson’s, neuroprotection refers to any intervention which delays or prevents the death of dopamine-producing cells and, therefore, slows or halts disease progression.
The best-known neuroprotection strategies are currently:
CONVENTIONAL THERAPIES
How can occupational therapy help?

Managing daily tasks become difficult in disease progression. An occupational therapist can help with:
How can a physical therapist help?
The key aims of physiotherapy in Parkinson’s are to help you:
Maintain a safe walking pattern/ gait (with or without mobility aids).
Maintain and improve functional ability and independence.

How can a speech and language therapist help?
It has been estimated that speech problems affect around 90% of people with Parkinson’s, from slurred speech to limited facial expressions, and a weak or quieter voice.
Parkinson’s speech therapy will help you overcome these communication difficulties, and also help with the many eating, swallowing or drooling problems that people with Parkinson’s may experience, like difficulty taking your medication, chewing issues, or producing too much or too little saliva.
A speech and language therapist can offer a range of treatments to help, including:
(https://parkinsonseurope.org/i-have-parkinsons/treatment/)
Multi-disciplinary team approach in the management of PD also includes the role of dietician and psychological counselling.
Dietary management to improve nutritional intake by eating energy-rich foods, the use of nutritional supplements and how diet can ease symptoms such as constipation.
Psychological counselling can help improve symptoms of anxiety and depression specially during early stages of disease.
To get more personalized answers,
download now


Your trusted health companion, delivering personalized and precise answers in real-time, ensuring informed decisions for a healthier you