What is dizziness?
Healthcare providers describe dizziness as having impaired or disturbed spatial orientation. Feeling woozy, lightheaded or a need to sit down in anticipation of fall, may be associated with dizziness. Frequent or severe dizziness may affect quality of life. People experience dizziness in different ways which may include:
Dizziness is a common complaint among the elderly, with as much as 30% of the population of older adults reporting dizziness with increased prevalence in women compared to men. Dizziness and associated postural imbalance have been shown to increase the risk of falls, with a resulting significant impact on quality of life, mortality, and the economic burden of associated costs. (https://www.ncbi.nlm.nih.gov/books/NBK572153/)
What are the causes of dizziness?
Inner ear disorders:
Labyrinthitis
Other causes may include:
What are the tests for patients presenting with dizziness?
Examination by the healthcare provider may show:
Following tests may be required to arrive at a diagnosis for patients presenting with dizziness:
What’s the difference between vertigo and dizziness?
The terms are often used interchangeably – but there are important differences.
Put in simple terms, “dizziness” is an umbrella term that covers a spinning, lightheaded, unbalanced or woozy sensation. The term “vertigo” is a specific form of dizziness in which you experience a spinning sensation – you either feel like your surroundings are moving around you, or that you’re moving. It is usually, but not always, caused by an inner ear problem.
Dizziness can become a serious issue as you age, contributing to falls and potential injuries, and can become debilitating.
How can a physical therapist help treat vertigo?
Vestibular rehabilitation therapy (VRT) is physical therapy that helps to reduce or eliminate balance and vertigo issues. Studies show people with balance issues who have VRT have improved balance, less dizziness and reduce their risk of falling.
Vestibular hypofunction has an estimated prevalence of 35.4% within the United States (US) adult population, with dizziness and postural imbalance noted as primary complaints. Research has indicated moderate to strong evidence to support exercise-based rehabilitation of the vestibular system as an effective treatment in populations including unilateral and bilateral vestibular hypofunction. It has shown promising research in treatments for central vestibular hypofunction. (https://www.ncbi.nlm.nih.gov/books/NBK572153/)
Who can benefit from VRT?
Dizziness may be a symptom of certain medical conditions that also affect your sense of balance. Dizziness and balance issues may also cause muscle fatigue and headache. Vestibular rehabilitation therapy may help people with conditions including:
The goals of vestibular rehabilitation therapy are: (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3259492/)
Enhancing gaze stability: Gaze instability is due to the decreased gain of the vestibular response to head movements. The best stimulus for increasing the gain of the vestibular response is the error signal induced by retinal slip, which is the image motion on the retina during head motion. Retinal slip can be induced by horizontal or vertical head movements while maintaining visual fixation on a target. The target can be placed either within an arm's length or across the room. Repeated periods of retinal slip induce vestibular adaptation. However, not all head movements result in a VOR gain change. Horizontal and vertical head movements are effective, whereas head movements in the roll plane do not induce sufficient changes in the VOR gain.
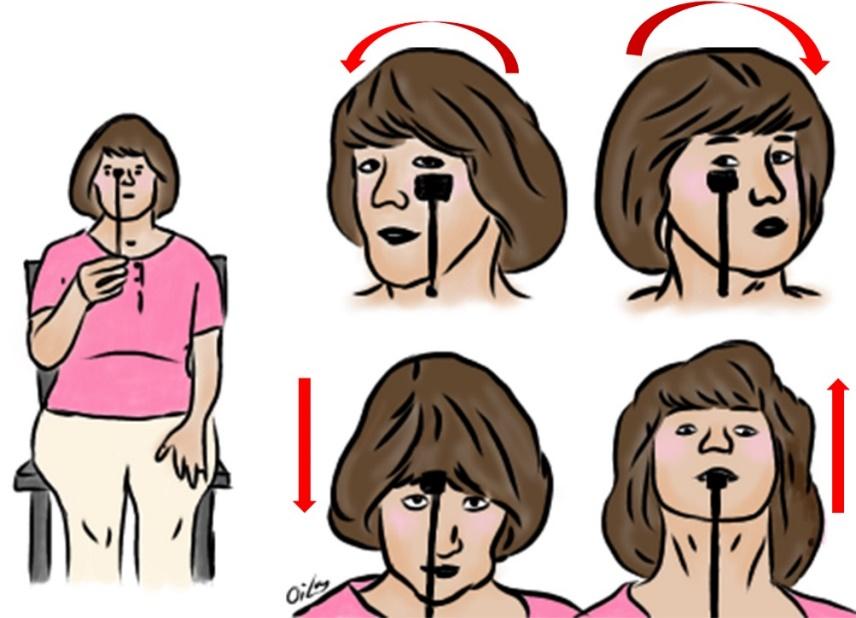
Patients should perform exercises for gaze stability four to five times daily for a total of 20-40 minutes/day, in addition to 20 minutes of balance and gait exercises. During the exercises to induce retinal slip, good visual inputs-such as bright room lights or with the curtains open-should be encouraged.
Enhancing postural stability: Postural stability recovery is slower than gaze stability recovery. The primary mechanisms of postural recovery are increasing reliance on the visual and somatosensory cues (substitution) and improving the vestibular responses (adaptation). Recovery of normal postural strategies is required in patients with temporary deficits, while cases of permanent vestibular deficits need compensatory strategies, such as relying on alternative somatosensory cues. The goals of VRT, especially for postural stability, are to help patients to a) learn to use stable visual references and surface somatosensory information for their primary postural sensory system, b) use the remaining vestibular function, c) identify efficient and effective alternative postural movement strategies, and d) recover normal postural strategies. For these, the therapist should assess whether the vestibular deficit is unilateral or bilateral, whether there is remaining vestibular function, whether the patient is overly reliant on particular sensory modalities such as vision or proprioception, and whether any other sensory impairment is present.
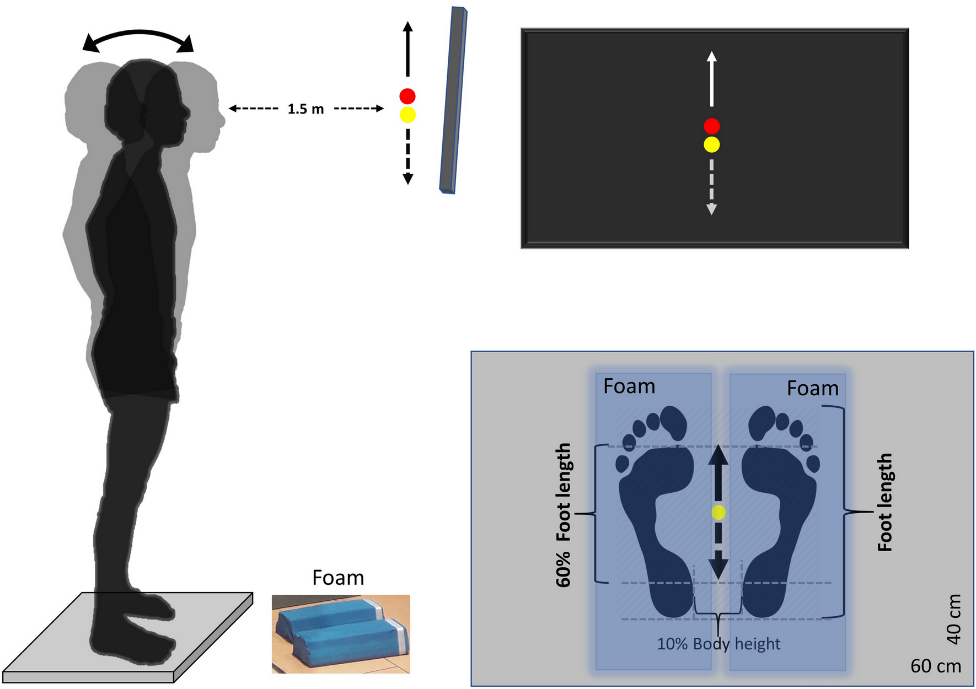
The Clinical Test for Sensory Interaction in Balance was designed to assess how sensory information from the vestibular, visual, and somatosensory systems is used for postural stability.
Improving activities of daily living: To achieve the final goal of vestibular recovery, the exercise is integrated into normal activities such as walking, rather than being performed with the patient sitting or standing quietly. Various games can be introduced to reduce the monotony of purely remedial exercises. For many, a more strenuous program is suggested that may include jogging, walking on a treadmill, doing aerobic exercises, or bicycling. Activities that involve coordinated eye, head, and body movements such as golf, bowling, handball, or racquet sports may be appropriate. Swimming should be approached cautiously because of the disorientation experienced by many vestibular patients in the relative weightlessness of the aquatic environment. Older adults who talk as they walk with assistive devices are more likely to fall than those who do not talk as they walk. Therefore, older patients should be instructed that when a conversation is started, they should stop walking in order to prevent falling. If rapid head movements cause imbalance, the patients should be advised not to drive.

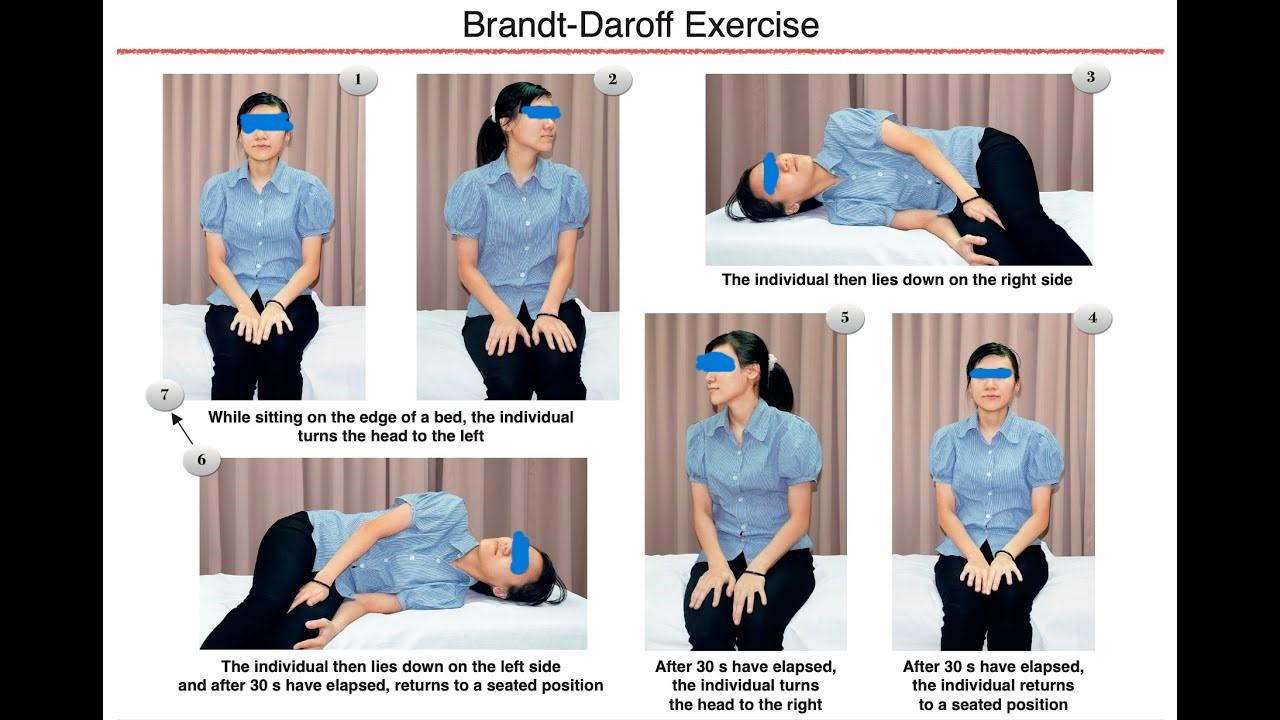
Improving Vertigo: Improving the vertigo should be the primary goal in most patients with provoked positioning vertigo without a definite diagnosis but with a benign aetiology. This can be achieved by habituation of abnormal vestibular responses to rapid movements. The therapist identifies the typical movements that produce the most intense symptoms and provides the patient with a list of exercises that reproduce these movements. The motion sensitivity test is used to assess the positions and movements that provoke symptoms. This test employs consecutive movements and positions such as turning the head or body during lying, sitting, or standing. Habituation is a reduction in the magnitude of the response to repetitive sensory stimulation, and it is induced by repetitive exposures to a provoking movement. Habituation is specific to the type, intensity, and direction of the eliciting stimuli. The Brandt-Daroff exercise is also a habituation therapy.
Patients who are gradually and safely exposed to a wide variety of sensory and motor environments are teaching their nervous systems to identify strategies to accomplish functional goals.
