Plantar fasciitis (PF) is the most common cause of heel pain. There are approximately 1 million visits annually in outpatient clinics presenting with the condition (Benjamin et al 2022). It accounts for 15% of all adult foot complaints requiring professional care and is prevalent in both athletic and non-athletic populations (Rome et al 2008). The peak incidence among the general population is between 40 to 60 years (Nahin et al 2018). Patients with limited ankle dorsiflexion, runners and workers with prolonged weight bearing job history can be prone to developing PF. Bilateral plantar fasciitis may be present in a third of cases with slightly higher prevalence in women compared to men and people with body mass index (BMI) greater than 25 kg/m2 (Lapidus et al 1965).
Where is plantar fascia?
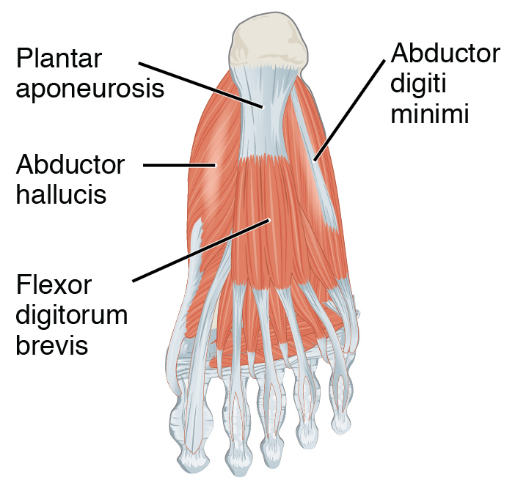
The plantar fascia or the plantar aponeurosis is a thick connective tissue that supports the arch of the foot. It originates from the calcaneal tubercle and extends into the forefoot dividing into medial central and lateral parts. The medial part attaches to abductor hallucis, and lateral part attaches to abductor digiti qunti pedis. The central thicker part divides into five bundles which attach to proximal phalanges through plantar plates.
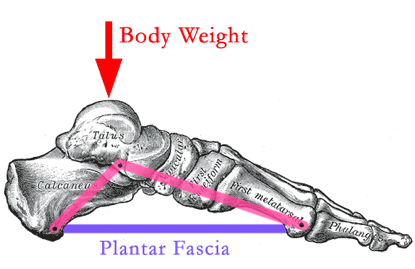
In normal gait cycle during mid-stance, the foot acts as a rigid lever to propel the body forward which is enabled by the stiffening of the plantar fascia. During push-off stage, the metatarsophalangeal joint extends which further tightens PF by the Windlass mechanism, initially described by Hicks in 1954.
What is plantar fasciitis?
Plantar fasciitis is often an overuse injury primarily due to repetitive strain causing degeneration and microtears of the fascia. It is peculiarly characterized by the presence of fibroblasts rather than inflammatory cells (Khan et al 2000, Lemont et al 2003). The plantar fascia plays an essential role in normal biomechanics of the foot by providing arch support and shock absorption while weight bearing. The most common symptoms are pain and stiffness in the heel, particularly during initial few steps. It is known to get exacerbated with prolonged weight bearing, impact activities like running, extension at big toe, barefoot walking specially on uneven surfaces which puts greatest strain on the fascia.
How to confirm the diagnosis?
Tenderness is reported by the patient during palpatory exam at the calcaneal insertion of the fascia. Patient has restricted ankle and big toe dorsiflexion which is often associated with pain. Windlass test is usually positive which helps to rule in the diagnosis of PF.

If conservative management fails to address symptoms, patients are usually referred for imaging. X-rays and ultrasound may show calcification in soft tissue or heel spur on the inferior aspect of calcaneum (Cho et al 2022). MRI can detect microtears, stress fractures or osteochondral defects that might be contributing to patient symptoms.

The Foot and Ankle Ability measure (FAAM) is a self-reported outcome measure which assesses the level of functioning in activities of daily living and sports related participation.
The physical therapist may additionally assess the accessory movements within the talo-crural joint, talo-calcaneal joints and perform soft tissue examination around the affected ankle and foot.
What is the treatment for Plantar Fasciitis?
Treatments are largely conservative and efficacious, with 90-95% of patients experiencing resolution of symptoms within 12-18 months. Activity modification to decrease cyclical repetitive loading of the plantar fascia should be advised during the treatment phase regardless of the chosen treatment modality (Lim et al 2016).
Initial treatment is directed at eliminating known risk factors that may have contributed towards symptom development.
Use of night dorsiflexion splints have produced highly positive outcomes (Batt et al 1996). However, patient adherence to using the splints may be a limitation as they may be cumbersome to have them on during the night (Powell et al 1998, Barry et al 2002).

Rolling foot on an ice bottle or can and oral NSAIDs can be used as adjuncts to manage pain. A randomized control trail comparing effects of NSAIDs and placebo showed no significant difference in pain and disability scores, considering the fact that PF is not an inflammatory process. Deep friction massage of the fascia can also help as an adjunct to improve circulation in the foot and promote healing.

Results of a 2008 query of orthopedic surgeons who are foot and ankle specialists showed that for patients with more than 4 months of pain, 74 out of 116 surgeons preferred PF-specific stretching and supervised physical therapy over anti-inflammatories or corticosteroid injections (DiGiovanni et al 2012). The plantar fascia-specific stretch has been shown to be more effective than the isolated Achilles stretching program (DiGiovanni et al 2006).

If patient continues to have moderate to severe symptoms that limit activities after 4-6 months of conservative therapy, referral for invasive intervention can be considered.
How can a physical therapist help?
Mobilizing metatarsophalangeal, subtalar and talocalcaneal joints helps reduce excess tensioning of the PF particularly in pes cavus foot deformity (Nawoczenski 1998).
Therapeutic ultrasound and soft tissue techniques can improve plantar fascia extensibility (Bolgla et al 2004).
Kinesiotaping helps support the foot to optimize ligament and muscle function that can help decrease the tensile forces placed on PF (Ross A 2003).

Strengthening of tibialis posterior, flexors of the foot, peronei that support controlled pronation and supination of the foot, thereby preventing over-loading of PF (Bolgla et al 2004).



It is also important to include strengthening of gluteus medius, gluteus minimus, TFL and Quadricep muscles. Weakness in these muscles inhibits their ability to assist with lower extremity load response, which results in greater transmission of shock to the supporting foot structures (Backstrom et al 2000).
Stretching the gastrocnemius and soleus is most frequently recommended in literature as improved Achilles tendon flexibility reduces the tension applied directly to plantar fascia (Viel et al 1989, Pfeffer et al 1999, Cornwall et al 1999).


To get more personalized answers,
download now


Your trusted health companion, delivering personalized and precise answers in real-time, ensuring informed decisions for a healthier you