CERVICOGENIC HEADACHE
What is cervicogenic headache (CGH)?
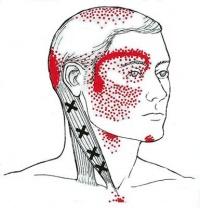
A cervicogenic headache presents as unilateral pain that starts in the neck and is referred from bony structures or soft tissues in the cervical spine. It is a common chronic and recurrent headache that usually starts after neck movement. It is usually accompanied by reduced range of movement of the neck. It could be often confused with migraine, tension headache or other primary headache syndromes. Diagnostic criteria must include all of the following points:
What is the pathophysiology of CGH?
CGH is thought to be referred pain arising from irritation caused by cervical structures innervated by spinal nerves C1, C2 and C3. Therefore, any structure innervated by the C1-C3 spinal nerves could be the source of CGH.
The C1-C3 nerves relay pain signals to the nociceptive nucleus of the head and neck, the trigeminocervical nucleus. This connection is thought to cause referred pain to the occiput and/or eyes. Aseptic inflammation and neurotransmission within the C-fibers caused by cervical disc pathology are thought to produce and worsen the pain in CGH.
The trigeminocervical nucleus receives afferents from the trigeminal nerve and the upper 3 cervical spine nerves. Neck trauma, whiplash, strain or chronic spasm of the scalp, neck or shoulder muscles can increase the area`s sensitivity similar to the allodynia seen in chronic migraines. A lower pain threshold makes patient more susceptible to more severe pain. For this reason, early diagnosis and therapeutic intervention are very important.
About 70% of CGH cases involve pathology of C2-3 zygapophyseal joint.
What is the epidemiology of CGH?
CGH is a rare condition that appears in people between the age of 30-44 years. Its prevalence among patients with headaches is 0.4 to 4 % affecting males and females nearly equally with the ratio of 0.97 (F/M). (https://www.ncbi.nlm.nih.gov/books/NBK507862/#:~:text=A%20cervicogenic%20headache%20presents%20as,of%20motion%20of%20the%20neck.)
What are the symptoms of CGH?
One sign of CGH is pain that comes from a sudden movement of neck. Another is, a headache that comes from the neck remaining in the same position for some time. Other signs may include:
What causes CGH?
Because CGH arise from problems in the neck region, different conditions can trigger this type of pain. These include:
How is CGH diagnosed?
History of patient`s symptoms is taken followed by physical examination of the head and neck. Range of movements are tested to reveal restrictions and stiffness. Patient is less likely to complain about sensitivity to light or noise such as in migraine.
Manual assessment of the upper cervical segmental mobility and pain has good reliability, with positive findings (pain produced with passive mobilization) in 63% of CGH patients and sensitivity of 80% as per study done by Page in 2011. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3201065/)
Imaging of the cervical spine is not sensitive enough to diagnose CGH. MRI, CT or CT myelography can be ordered to rule out Chiari malformations, nerve root pathology assessment or identify spinal cord pathology.
The ICHD-3 criteria for cervicogenic headache are as follows:
Diagnostic anaesthetic blocks can sometimes be utilized to confirm the diagnosis but require specialized skills and are not routinely performed.
What is the treatment for CGH?
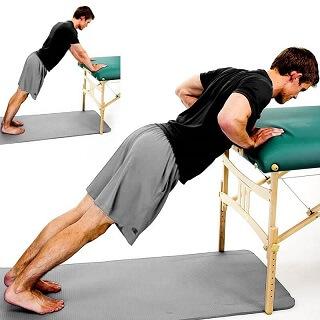
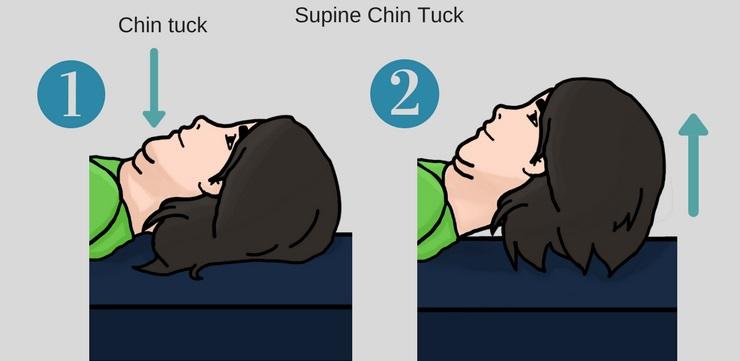
Strengthening of deep neck flexors and scapular stabilizer exercises, in addition to upper cervical extensor stretching are advocated in the treatment of CGH. (https://www.ncbi.nlm.nih.gov/books/NBK507862/#:~:text=A%20cervicogenic%20headache%20presents%20as,of%20motion%20of%20the%20neck.)
Nerve block: this may temporarily relieve pain and help work with physical therapy.
To get more personalized answers,
download now


Your trusted health companion, delivering personalized and precise answers in real-time, ensuring informed decisions for a healthier you