Commonly known as frozen shoulder, Adhesive capsulitis of shoulder is an inflammatory condition characterized by shoulder pain, stiffness and loss of active and passive range of movements (St Angelo et al 2023). It affects 5.3% of population with the average duration of 1 to 3.5 years (Ryan et al 2016). The mean age of symptom occurrence has been found to be 55 years and the prevalence is slightly more in females.
Etiology
Primary adhesive capsulitis is idiopathic and has gradual onset. It is commonly associated with underlying conditions such as diabetes mellitus, thyroid disease, hypertriglyceridemia and/or cervical spondylosis (Small et al 2018)
Secondary adhesive capsulitis is typically the result of trauma such as tears of rotator cuff, fractures, surgery and/or immobilization or underlying conditions like diabetes, thyroid disorders, stroke, etc. (Le HV et al 2017)
The condition goes through 3 stages (Le HV et al 2017) –
Arthroscopic studies of the affected shoulder show the following histopathological findings (Patel et al 2020) (Tao et al 2017) (Tamai et al 2014)
Evaluation
Painful and reduced gleno-humeral joint range of movements are predominant findings in adhesive capsulitis. Active and passive ranges are significantly restricted in two or more planes when compared with the unaffected shoulder. Range of movement (ROM) restriction usually follows the capsular pattern where external rotation is first and most restricted followed by abduction and internal rotation (Rundquist et al 2003).
Accessory movements of the gleno-humeral joint are most restricted for which the scapulo-thoracic joint compensates in achieving higher range of movements during physical examination.
Neer`s impingement and Hawkin Kennedy tests for shoulder impingement are often positive. In primary adhesive capsulitis lab testing may not reveal abnormalities however, in secondary adhesive capsulitis lab testing may be required to find the underlying pathology.
X-ray may be considered in case of suspicious calcification of the tendons or fractures. MRI may reflect the histopathologic changes of the joint space, synovium, capsule and/or surrounding soft tissue structures.
Treatment of Primary adhesive capsulitis
Stage 1 -
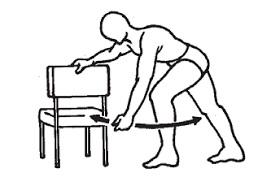
Maintenance of ROM and pain reduction are the most important part of care during the initial stage. Following are few exercise examples that are active and/or active assisted that can serve to preserve gleno-humeral movements (Check & Cohen 2015)
Educating the patient about the stage progression, advice on activity modification to reduce irritability can significantly help with pain reduction and compliance with therapy.
Pain neuroscience education and graded motor imagery can be used to address central sensitization. Intensive therapy in the inflammatory stage could be detrimental to long term outcomes (Sawyer et al 2018)
Few studies support the use of hot packs, therapeutic ultrasound and electrical stimulation for pain reduction (Kelley et al 2013)
There is controversial evidence in role of manual therapy and joint mobilizations to treat adhesive capsulitis (Zavala – Gonzales et al 2018) especially in freezing stage likely pointing to tissue irritability, hence resorting to tailor made method of treatment application (Duenas et al 2019). Vigorous rehab needs to be avoided as it has known to cause worsening of symptoms (Vermeulen et al 2006)
Stage 2
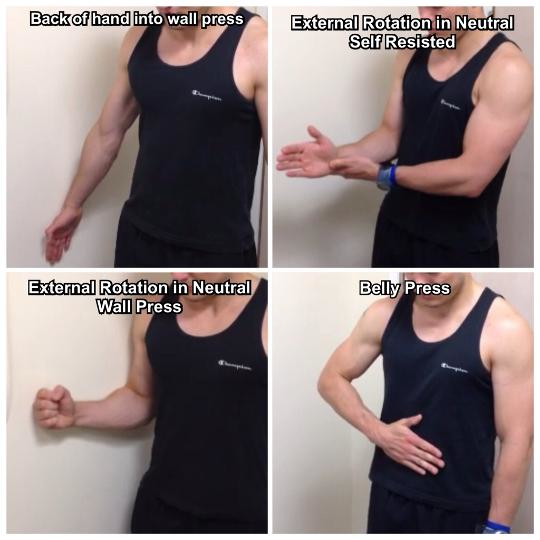
Patient can exhibit higher levels of pain and/or stiffness in frozen stage. Depending on tissue irritability, the exercise dose and intensity can be either sustained as in stage 1, or progressed. Below 90°degree angular exercise stretches and gentle isometric strengthening to enhance scapular stability can be gradually introduced as tolerated (Chan et al 2017). Following are examples of basic exercises that can be introduced in stage 2
Full Range Active Assisted Shoulder Flexion

Various studies have showed benefits of intra-articular steroid injection for adhesive capsulitis preferably in early stages (Bulgen et al 1984). Injection combined with shoulder mobility and stretching exercises are more effective in providing short term pain relief and improved function compared to shoulder mobility and stretching exercise alone (Kelley et al 2013). Multiple injections can be considered to provide symptomatic relief (Hettrich 2016) (Shahzad et al 2021)
Stage 3
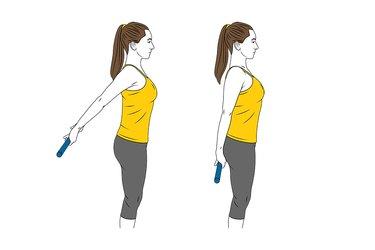
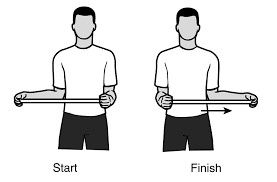
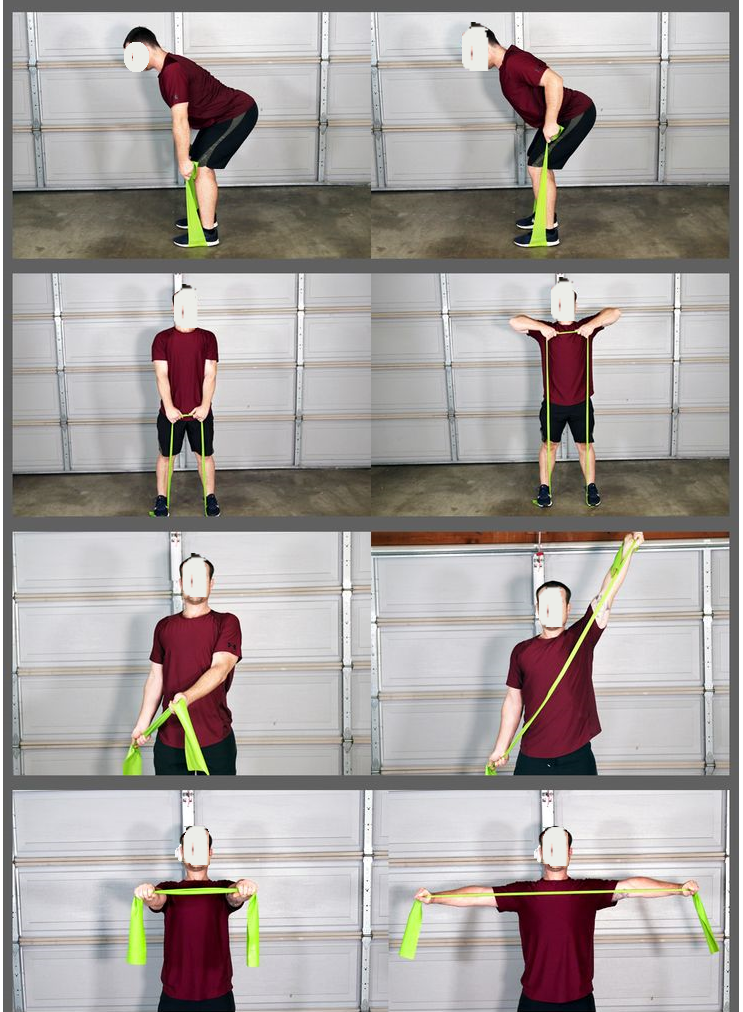
This stage is usually characterized with stiffness as a primary symptom and better tolerance to progression of exercises. At this stage the range of movements can be progressed to angles beyond 90° if well tolerated. Introduction of resistance bands from inner to outer angles progressively can help restore normal shoulder functions. Examples of basic exercises suitable for stage 3.
In case of severe functional limitations and poor recovery, surgical intervention can be an option for some patients in the form of manipulation under anesthesia, arthroscopic or open capsular release (Grant et al 2013) (Smitherman et al 2015) (Lee et al 2020).
Treatment of Secondary adhesive capsulitis
Occurrence of secondary adhesive capsulitis can be attributed to various known underlying primary causes such as Diabetes, thyroid, stroke, trauma, surgical intervention, immobilization, etc. Patients with low to moderate levels of irritability are ideal candidates for rehab. Therapeutic exercises and mobilizations are highly recommended for pain reduction and improving ROM (Jain & Sharma et al 2014)
The physical therapist evaluates pain, stiffness, tissue irritability and function based on which joint mobilization grades are applied. Grades I & II are predominantly used for pain relief whereas grades III, IV and V are used to achieve increase ROM goals.
The therapist may apply joint mobilizations to the sterno-clavicular joint, acromio-clavicular joint, scapulo-thoracic joint and gleno-humeral joint of the shoulder complex to achieve mobility goals.
Adding rotator cuff strengthening and scapular stabilizing exercises rather than using joint mobilizations alone are shown to improve outcomes (Rawat et al 2017).
Proprioceptive neuromuscular facilitation exercises have been proved to be effective in increasing ROM and decreasing pain (Tedla et al 2019, Chan et al 2017, Shabbir et al 2021)
Surgery can be indicated in patients who do not respond to physical therapy, intra-articular injection or oral drugs like NSAIDS or steroids (Arse et al 2015)