The medications and treatments used vary depending on the type of stroke and how soon a person receives treatment after the stroke. There are also long-term treatments for stroke. These happen in the days and months after emergency treatment deals with a stroke’s immediate threat.
ISCHEMIC STROKE
HEMORRHAGIC STROKE
Thrombolytic drugs (within three to four and half hours)
Blood pressure management
Thrombectomy (within 24 hours if there is no significant brain damage)
Reversal of any medication that might increase bleeding
Blood pressure management
Use of medications or surgery to reduce pressure inside the skull
Surgical procedures are aimed to remove blood or blood clots and open up blocked arteries restricting blood flow to the brain.
Your healthcare professional may recommend one of these procedures if an aneurysm, arteriovenous malformation (AVM) or other blood vessel condition caused the stroke.
Surgical clipping. A surgeon places a tiny clamp at the base of an aneurysm to stop blood flow to it. An aneurysm is a bulge at a weak spot in a blood vessel. The clamp can keep the aneurysm from bursting. Or the clamp can keep an aneurysm that has recently burst from bleeding again.
Coiling, also known as endovascular embolization. A catheter is inserted into an artery in the groin and guided to the brain. Using the catheter, a surgeon places tiny coils into the aneurysm to fill it. This blocks blood flow into the aneurysm and causes blood to clot.
Surgical removal of a tangle of thin-walled blood vessels, known as an AVM. Surgeons may remove a smaller AVM if it's in an area of the brain that's easy to access. This removes the risk of rupture and lowers the risk of haemorrhagic stroke. However, it's not always possible to remove an AVM if it's deep within the brain or if it's large. It also may not be possible to remove if the procedure would impact brain function.
After emergency treatment, you're closely monitored for at least a day. After that, stroke care focuses on helping you recover as much function as possible and to return to independent living. The impact of the stroke depends on the area of the brain involved and the amount of tissue damaged.
If the stroke affected the right side of the brain, movement and feeling on the left side of your body may be affected. If the stroke damaged the left side of the brain, movement and feeling on the right side of your body may be affected. Brain damage to the left side also may cause speech and language disorders.
Most people who have had a stroke go to a rehabilitation program. Your healthcare professional can recommend the therapy program that is right for you. A program is recommended based on your age, overall health and degree of disability from the stroke. Your lifestyle, interests, priorities and whether you have help from family members or caregivers are considered.
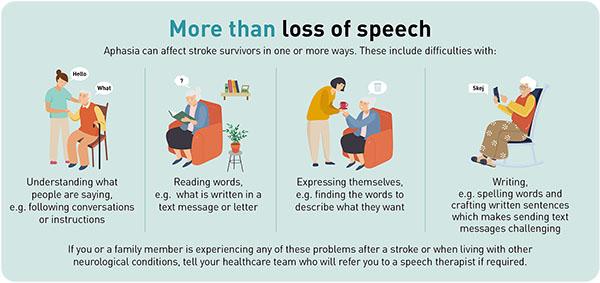
If you have aphasia, your rehabilitation program may include practising talking, listening, reading or writing. You may work with the speech pathologist on your own or in a group. You may use a computer to work through exercises. You may practise using gestures or aids to get your message across.
If you have apraxia, treatment will focus on helping your muscles to work together. You may work on making sounds accurately and improving the speed and rhythm of your speech. You may practice using words and sentences that gradually get longer and more complex.
Occupational therapy: intervention improves participation in meaningful roles, tasks, and activities.
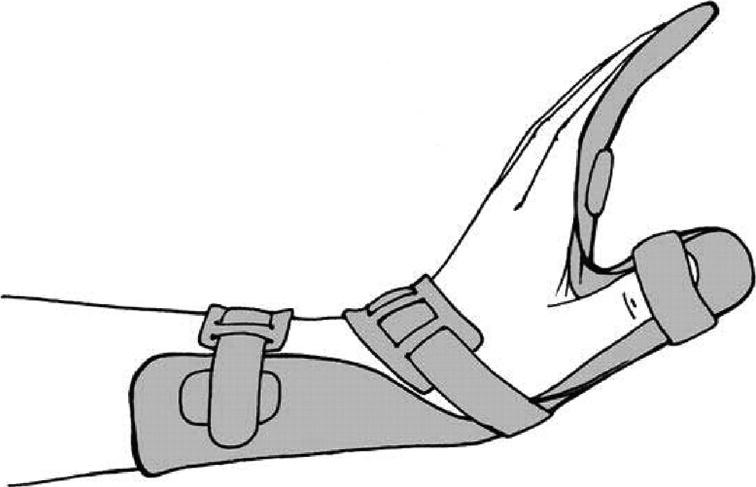
Static or dynamic splinting can be given to reduce spasticity with limb positioning to reduce oedema.
Supportive strapping can be used to reduce a subluxed shoulder or prevent further shoulder subluxation.
Visual and perceptual impairments are minimized by retraining in specific skills, teaching compensation techniques, substitution of unimpaired skills, or adapting the task or environment.
Occupational therapists will establish how tasks can be adapted or the environment changed to improve the patient's level of independence. For the physical environment, the occupational therapist may prescribe assistive equipment or home modifications to enable task performance with greater ease or safety. For example, installing grab rails near steps, raising the chair height, or prescribing a wheeled mobility tray for transporting meals. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9204113/)
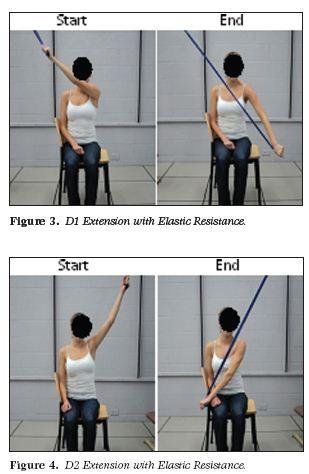
Physical therapy intervention strategies for stroke rehabilitation are divided as per the recovery stages.
Acute stage: Research has confirmed that early, organized stroke unit care reduces mortality rates, hospital stays, impairments, etc. The interventions are primarily concentrated on positioning, functional mobility training, ADLs training, ROMs, splinting, and bed mobility. Early mobilization after appropriate monitoring can help prevent the adverse consequences of bed rest and deconditioning, reduce mental deterioration, stress and anxiety, and improve the patient’s consciousness level. Furthermore, maladaptive movement patterns can be minimized through early mobilization.
Maintenance of anti -spastic/ antisynergistic posture.
Maintenance of Range of motion.
Maintenance of airways and facilitation of breathing.
Maintenance of muscle properties and strength.
Stimulation of upper limb, lower limb and Oro-facial function.
Facilitation of bed mobility such as lying to sitting.
Facilitation of early sitting and trunk control.
Facilitate transfers and ambulation training.
Research supports the use of conventional therapies such as therapeutic exercises and functional retraining, that are given in all stages showing significant improvement in outcome measures.
The primary goals of rehabilitation after stroke include being able to walk independently and to manage to perform daily activities. The aim of all physical therapies is to improve ADL’s, functional ambulation and independence. Specifically designed preparatory exercises, physical therapist’s observation and direct manipulation of the lower limbs position during gait over a regular surface, followed by assisted walking practice over ground.
Neurophysiological Approaches used for stroke rehabilitation: 1. Muscle Re-education Approach. 2. Neurodevelopmental Approaches: – Sensorimotor Approach (Rood, 1940S) – Movement Therapy Approach (Brunnstrom, 1950S) – NDT Approach (Bobath, 1960-70S) – PNF Approach (Knot and Voss, 1960- 70S) 3. Motor Relearning Program for Stroke (1980S) 4. Contemporary Task Oriented Approach (1990S) (https://www.ijhsr.org/IJHSR_Vol.8_Issue.5_May2018/51.pdf)
A multi-disciplinary team for stroke management may include a neurologist, physiatrist, rehabilitation nurse, dietician, recreational therapist, physical therapist, occupational therapist, speech therapist, social worker or case manager, psychologist or psychiatrist. (https://www.mayoclinic.org/diseases-conditions/stroke/diagnosis-treatment/drc-20350119)
Chronic stage: Community fitness programs are helpful and water-based exercises have been shown to improve function as per a 2007 study by Pollock et al. Aims of management in chronic stage include:
Sub-acute stage: After six months, patients who fell into this category are referred to inpatient rehabilitation or home rehabilitation. Interventions during this period include constraint-induced movement therapy, supportive walking that may be electromechanically assisted, and B/L training. A study by De Wit et al recommended that exercises can be scheduled for six days a week for three hours per day.
Active therapy and graded task selection is used to encourage sensorimotor return; the therapy may include muscle facilitation and strengthening, in conjunction with everyday activities to develop reach, grasp, and object manipulation skills. Examples of practice tasks include: using a keyboard, mobile phone, television remote, or calculator to practice fine motor skills; opening a range of jars and containers of varying sizes and weights and with different types of lids; turning the pages of books, magazines, and newspapers; and managing fastenings of clothing items with different-sized buttons, zippers, Velcro, clips, and laces. The occupational therapist reviews and upgrades the therapy program on a daily basis.
Speech therapy: Communication difficulties affect everyone differently. A speech pathologist will assess your talking, listening, reading, writing and understanding. They will work with you to develop a rehabilitation program to meet your needs and goals. They can suggest ways to communicate more easily, and aids that can help.