Osteoarthritis (OA) is a degenerative joint disease (DJD), in which the tissues in the joint break down overtime. It is the most common type of arthritis and is more common in older people. The most commonly affected joints include:
Hands
Knees
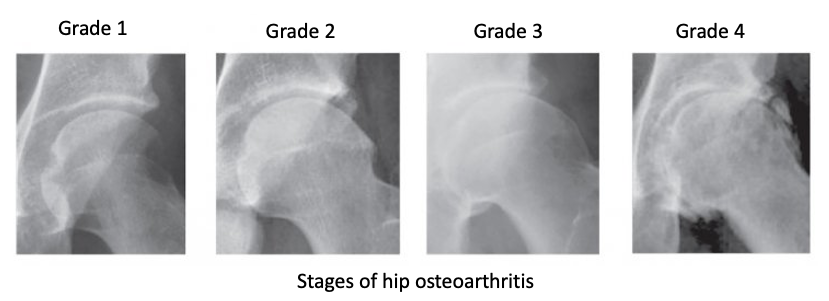
Hips
Neck
Lower back
For some people OA can be very mild and does not affect activities of daily living (ADL), compared to others who have severe pain and disability.
Who can get Osteoarthritis?
Anyone can get OA, however, it is more common as people age. Women are more likely to have OA, especially after 50 which can be associated with menopause. Younger people can develop OA usually as a result of joint injury, abnormal joint structure or congenital cartilage defect.
Other reasons may include being overweight, diabetic, having a history of surgery of same or adjacent joints affecting biomechanics, overuse due to occupation or family history of arthritis. (https://www.niams.nih.gov/health-topics/osteoarthritis)
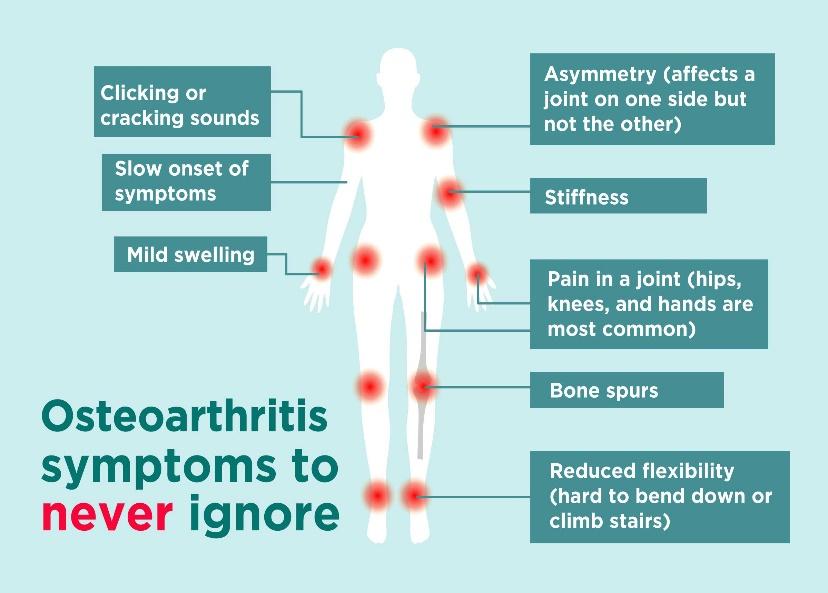
What are the symptoms of OA?
Symptoms of OA often develop slowly and worsen over time –
Pain – affected joints may hurt during or after movement and usually improve with rest. For some people in later stages, the pain may be worse at night.
Stiffness – can be most noticeable after waking in the morning or after being inactive.
Tenderness – can be felt with light pressure around the affected joint line.
Loss of range of movement – when attempting to move the joint to full range of movement.
Grating sensation – while moving the joint there might be a palpable “click” or “pop” or “crack”.
Bone spurs – are extra growths from the bone surface that can be felt like hard lumps.
Joint instability – and the feeling that the joint is “loose” and might give away with loading or an externally applied force.
Swelling, redness and warmth – are the signs of inflammation that can be noticed around the joint, specially after overuse.
What is the common pathophysiology of OA applicable to most typical joints of the body?
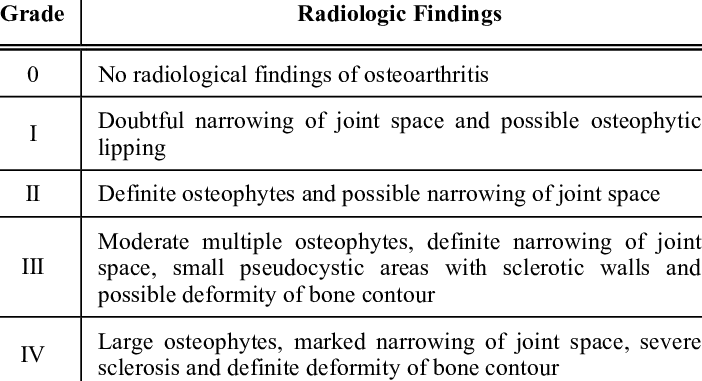
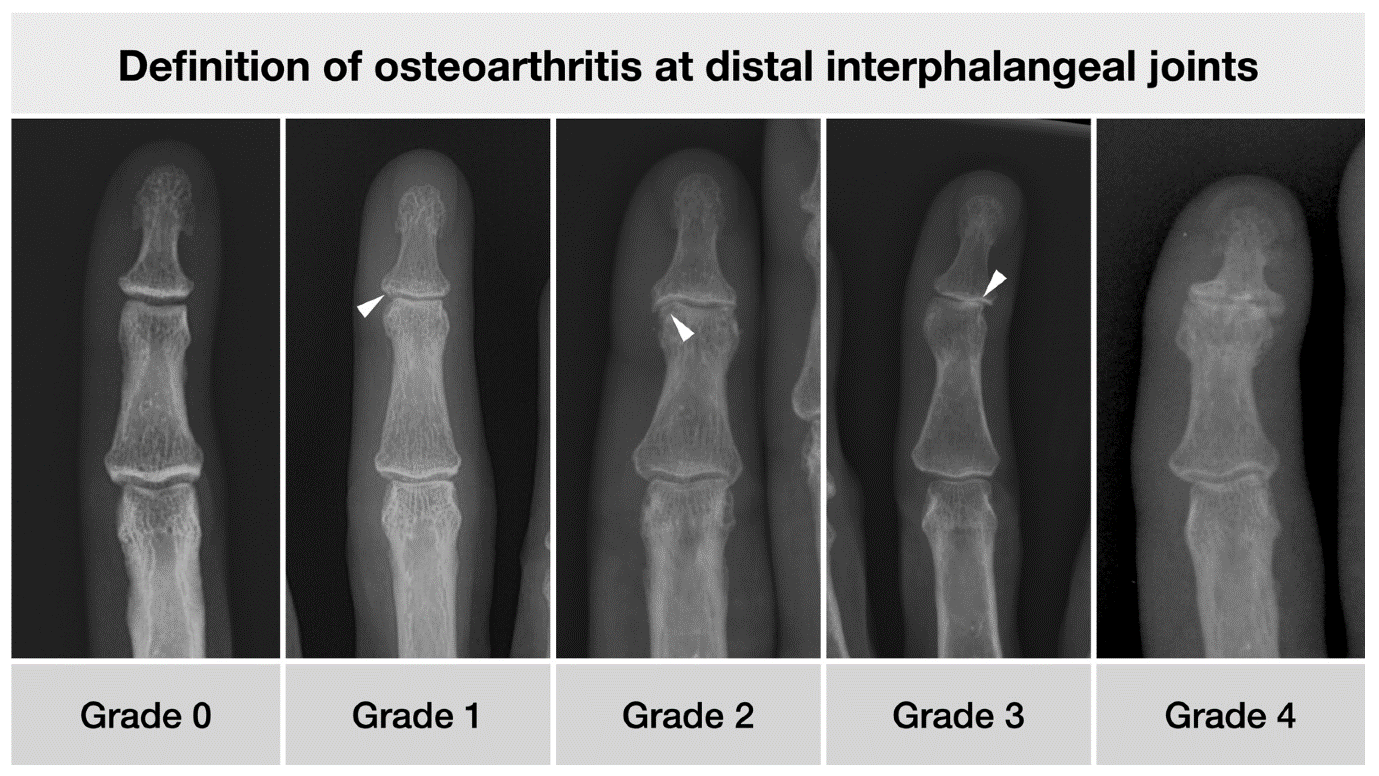
The pathophysiology of OA can be divided in to four stages.
Stage 1 (Mild) – there are mild symptoms clinically, like pain in the affected joint. The underlying cartilage is intact in this stage.
Stage 2 (Moderate) – cartilage shows signs of wear and tear on imaging and clinically patient experiences acute sharp pain associated with joint stiffness.
Stage 3 (Advanced) – joint pain, stiffness, swelling are more constantly present through most activities of daily living. Underlying cartilage is almost completely lost with significant loss of joint space.
Stage 4 (Severe) – Most patients present with severe pain and significant loss of joint movements. There is also significant amount of instability, muscle weakness and complete loss of cartilage. The underlying bone surface shows signs of sclerosis and there is complete loss of joint space.
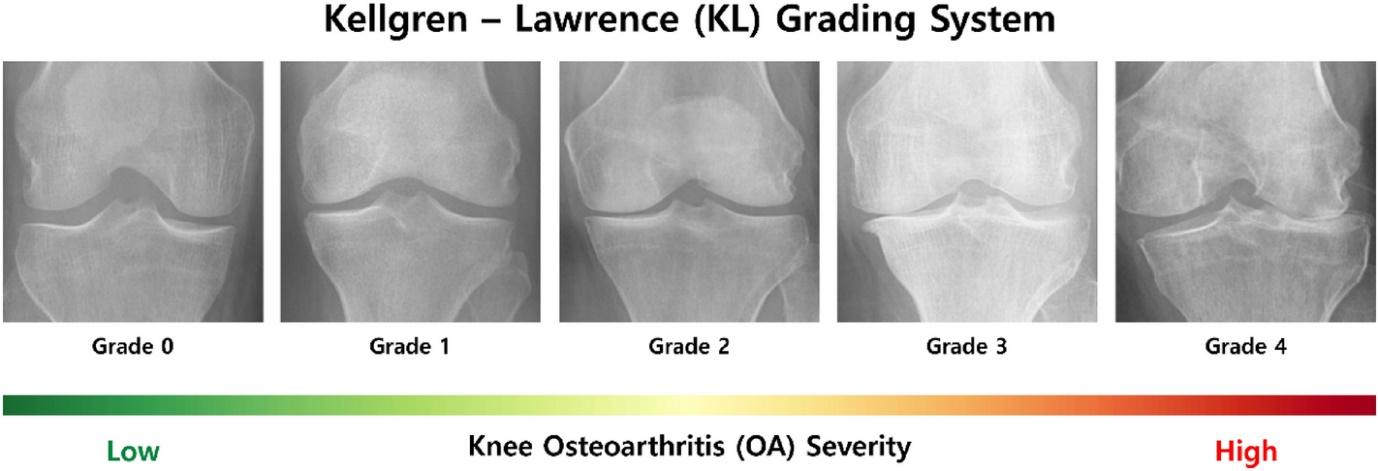
Knee OA
Knee is a tricompartmental joint. OA can affect one or more compartments at the same time. Typical presentation of OA knee include –
Worsening of knee pain particularly during or just after long walks, running, jogging, using stairs, kneeling.
Stiffness in knee after waking up in the morning or after a while of inactivity
Swelling around the knee joint – few patients may have “baker`s cyst” which is swelling on the back of the knee.
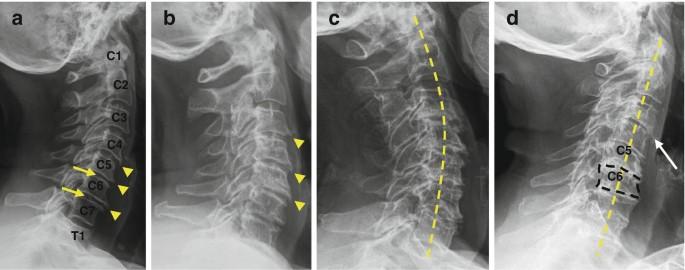
Also commonly known as cervical spondylosis, is characterized by degenerative changes to cervical vertebrae, disks, facet joints and soft tissues with aging.
Clinically patients present with neck pain and stiffness. The pain often radiates in the shoulder, arms or cause headache.
There is restriction of range of movements upon examination with “clicking” or “crepitus” during movements.
In a few cases, other than the usual musculoskeletal symptoms patients can present with neurological weakness in the arm, sensory deficits, vertigo or nausea.
In severe cervical OA, the intervertebral disk dehydrates thus narrowing the intervertebral space causing nerve root compression and radicular symptoms.
Lower back OA
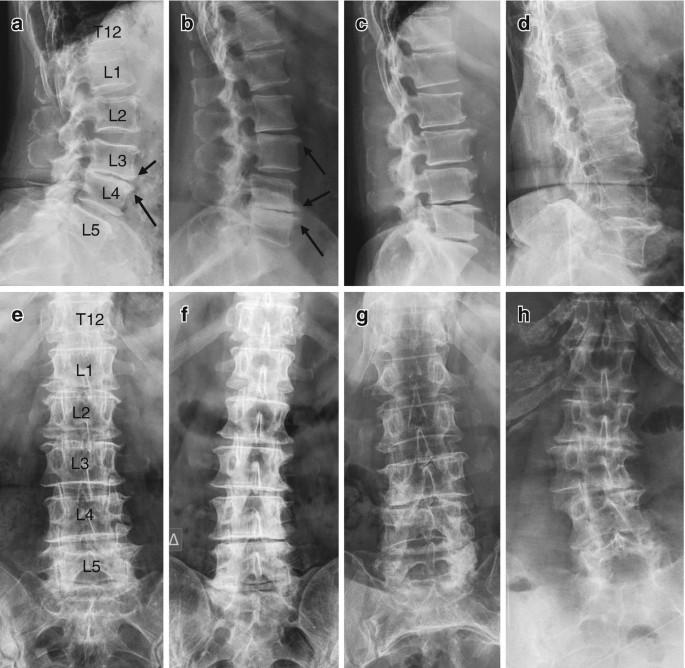
Also commonly referred as lumbar spondylosis or degenerative conditions of the spine.
Patients present clinically with lower back pain and stiffness which is worse in mornings and after joint overactivity.
Swelling and tenderness over the affected vertebrae.
In advanced degeneration, the intervertebral disk losses water and there is narrowing of intervertebral foramen causing nerve root compression and radicular symptoms.
Root compression may present with neurological symptoms in lower extremities like motor weakness or sensory deficits.
Patient may have a “limp” or altered walking pattern due to painful lower back which may involve lower limb referral.
In more advanced cases there may be a spinal deformity or a spinal list (shift of the spine towards non-painful side).
The process of diagnosing OA involves detailed history from the patient about symptoms, functional limitations, inquiry of other medical conditions, medications, clinical examination, lab tests and imaging. It is important to rule out other diagnosis like Rheumatoid arthritis, gout or infectious joint conditions.
What is the treatment of OA?
Osteoarthritis cannot be reversed, however treatments can help reduce pain and move better. It is always recommended to seek the physician`s advice before taking pain relief medication for managing OA.
Medications
Acetaminophen- (Tylenol) has been shown to give pain relief in mild to moderate osteoarthritis. Long term use of acetaminophen is linked to liver damage.
Non-steroidal anti-inflammatory drugs (NSAIDs) – such as Ibuprofen and Naproxen sodium taken at recommended doses relieve OA pain. Prescription is required for determining dosage as NSAIDs have the side effects like stomach upset, cardiovascular problems, bleeding, liver and kidney damage.
Duloxetine – (Cymbalta) is normally prescribed as an anti-depressant, but is also an approved drug to treat chronic pain including OA.
Education & awareness regarding the disease to avoid fear of movement and exercises. Identifying actual pain triggers and modifying activities to promote function effectively.
Pain relief – various modalities such as transcutaneous electrical stimulation, interferential currents, low level laser therapy or acupuncture have been shown to make some difference in the level of pain and function as per some evidence.
Acquire flexibility – of the muscles and soft tissues that impact the OA affected joint. This can involve the therapist either passively moving the joint or assisting the patient in performing the movement through the available range. The aim of exercise is to improve blood flow in the affected joint and reduce stiffness experienced during movements.
Muscle strengthening – can be performed by weights, resistance bands or even body weight working against gravity. Strong muscles not only help to support and protect joints, but also to enhance stability which is crucial in advanced OA when the joint surfaces lose congruency.
Aerobic exercises – when done regularly, such as bicycling, swimming or elliptical machine helps to keep body weight under control. Keeping check on body weight helps OA, specially in lower body due to less pressure on joints during weight bearing.
Gentle, non-impact activities or exercises like Tai-chi, aquatic aerobics and yoga are extremely beneficial in attaining all the therapy goals and retard the rate of joint degeneration.
The therapists can design braces or splints to support joints and improve joint alignment to minimize pain and discomfort during functional activities.
They can also help with assistive devices to facilitate mobility in cases of severe disability.
The therapists can also help with environmental modification at work and home to have adaptation strategies in place for better functional outcomes. For e.g. having handle bars near toilet to help standing back up, having a broad grip knife for better grip during chopping food, office chair and desk height modifications to have less strain on the spinal, shoulder or wrist joints.
Corticosteroid injections
These are given intra-articular, i.e. in the joint space with the aim of reducing the inflammation and provide pain relief.
There are a limited number of injections that can be administered to the patient as it can result in joint damage if given in excess.
Joint replacement surgery
Joint replacement is offered to patients who do not achieve desired outcomes with conservative management and have severe functional limitations.