Multiple sclerosis is a chronic autoimmune disease affecting the central nervous system (CNS) and is characterized by inflammation, demyelination, gliosis, and neuronal loss. Multiple sclerosis (MS) is the most frequently seen demyelinating disease, with a prevalence that varies considerably, from high levels in North America and Europe (>100/100,000 inhabitants) to low rates in Eastern Asia and sub-Saharan Africa (2/100,000 population). Knowledge of the geographical distribution of the disease and its survival data, and a better understanding of the natural history of the disease, have improved our understanding of the respective roles of endogenous and exogenous causes of MS. (https://pubmed.ncbi.nlm.nih.gov/26718593/)
What is the pathophysiology of MS?
MS refers to the formation of plaques in CNS along with inflammation, demyelination, axonal damage, and axonal loss. These plaques are located in the brain and spinal cord, mainly in the white matter surrounding the ventricles, optic nerves and tracts, corpus callosum, cerebellar peduncles, long tracts, and subpial area of the spinal cord and brainstem, as well as gray matter. Clinical symptoms characterized by acute relapses typically appear first in young adults, followed by a gradually progressive course leading to permanent disability within 10 to 15 years.
MS is likely the result of a complicated interplay between genetics, food, and the environment. MS is primarily caused by an autoimmune attack on the CNS due to hyper immunity. Numerous postulated pathways have been proposed, but the proposed "outside-in" mechanism involves CD4+ proinflammatory T cells. Researchers hypothesize that an unknown antigen promotes and activates 1 T-helper (Th1) and 17 T-helper (Th17), leading to CNS endothelium adhesion, blood-brain barrier (BBB) crossing, and subsequent immune attack through cross-reactivity. The "inside-out" theory posits that an innate malfunction of CNS produces and culminates in inflammation-mediated tissue destruction. The phenomenon of environmental impacts, such as latitudinal gradients in different countries, has been widely studied. A deficiency in vitamin D has been a possible explanation for susceptibility observed in populations living at higher latitudes. Individuals with relatives have a considerable chance of developing the disease. The expected range of heritability is between 35 and 75%. Human leukocyte antigen DRB1*1501 has a significant association with MS. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9888604/)
What is the classification o MS?
Multiple sclerosis presents various disease courses and is classified into 7 categories, as outlined below.
Additionally, the following 3 categories are sometimes considered within the spectrum of multiple sclerosis:
What are the risk factors to get MS?
Age, sex, race, heredity, geography, vitamin D deficiency, past injury to the nervous system, smoking and infections such as herpes simplex, chlamydia, and rabies are risk factors to get MS.
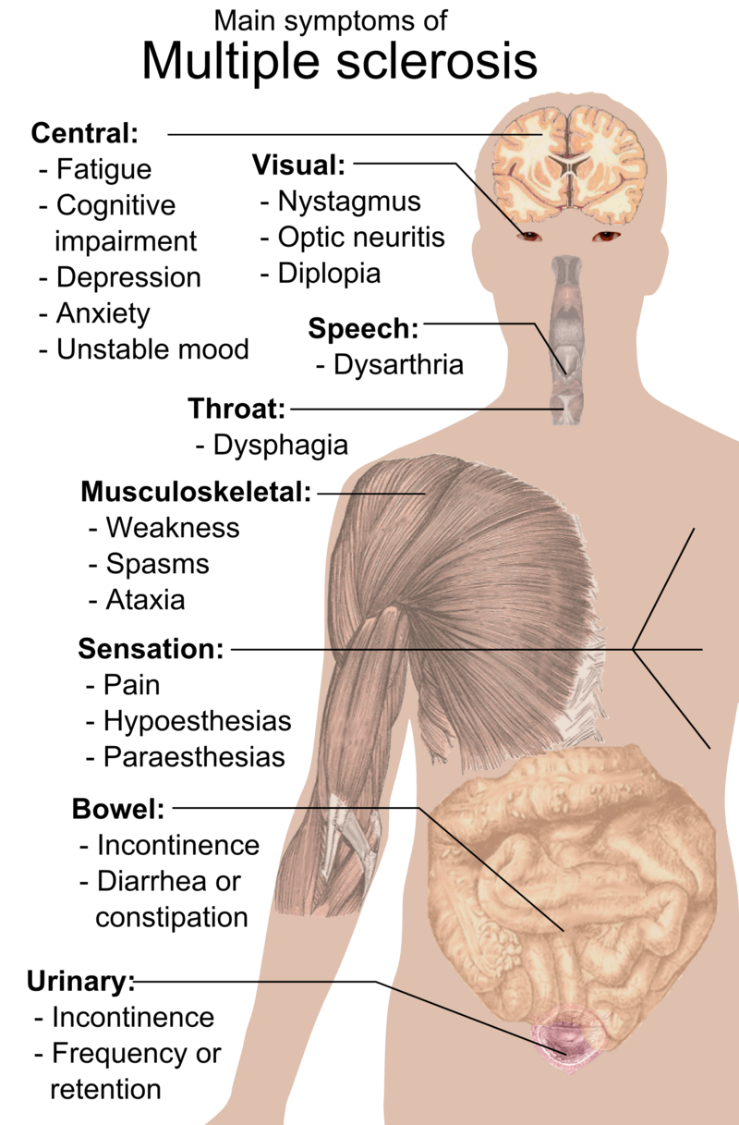
What are the symptoms of MS?
Multiple sclerosis signs and symptoms may differ greatly from person to person and over the course of the disease depending on the location of affected nerve fibres.
Common symptoms include:
Lack of coordination
(https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/symptoms-causes/syc-20350269)
What does the patient history and physical exam reveal in MS?
Multiple sclerosis presents with a broad range of symptoms reflective of the multifocal lesions of the CNS. The severity and diversity of symptoms are influenced by the burden, location, and extent of tissue injury. Interestingly, symptoms may not always align with MRI evidence of active plaques due to the involvement of repair mechanisms and neural plasticity in tissue injury and recovery processes.
Typical clinical manifestations noted in patient history include:
Features considered atypical for multiple sclerosis include seizures, steady progression of symptoms, deficits developing rapidly within minutes, onset before age 10 or after 50, rigidity or sustained dystonia, cortical deficits such as apraxia, alexia, aphasia, or neglect, and early onset of dementia.
The relapsing-remitting course of multiple sclerosis, observed in a majority of patients, is characterized by exacerbation and relapses of neurological symptoms, with stability between episodes. The following features generally characterize the relapsing-remitting course of multiple sclerosis:
Symptoms from relapses frequently resolve. However, over time, residual symptoms relating to episodes of exacerbation accrue. This accrual of symptoms, generally after 10 to 15 years, results in long-term disability over time. (https://www.ncbi.nlm.nih.gov/books/NBK499849/)
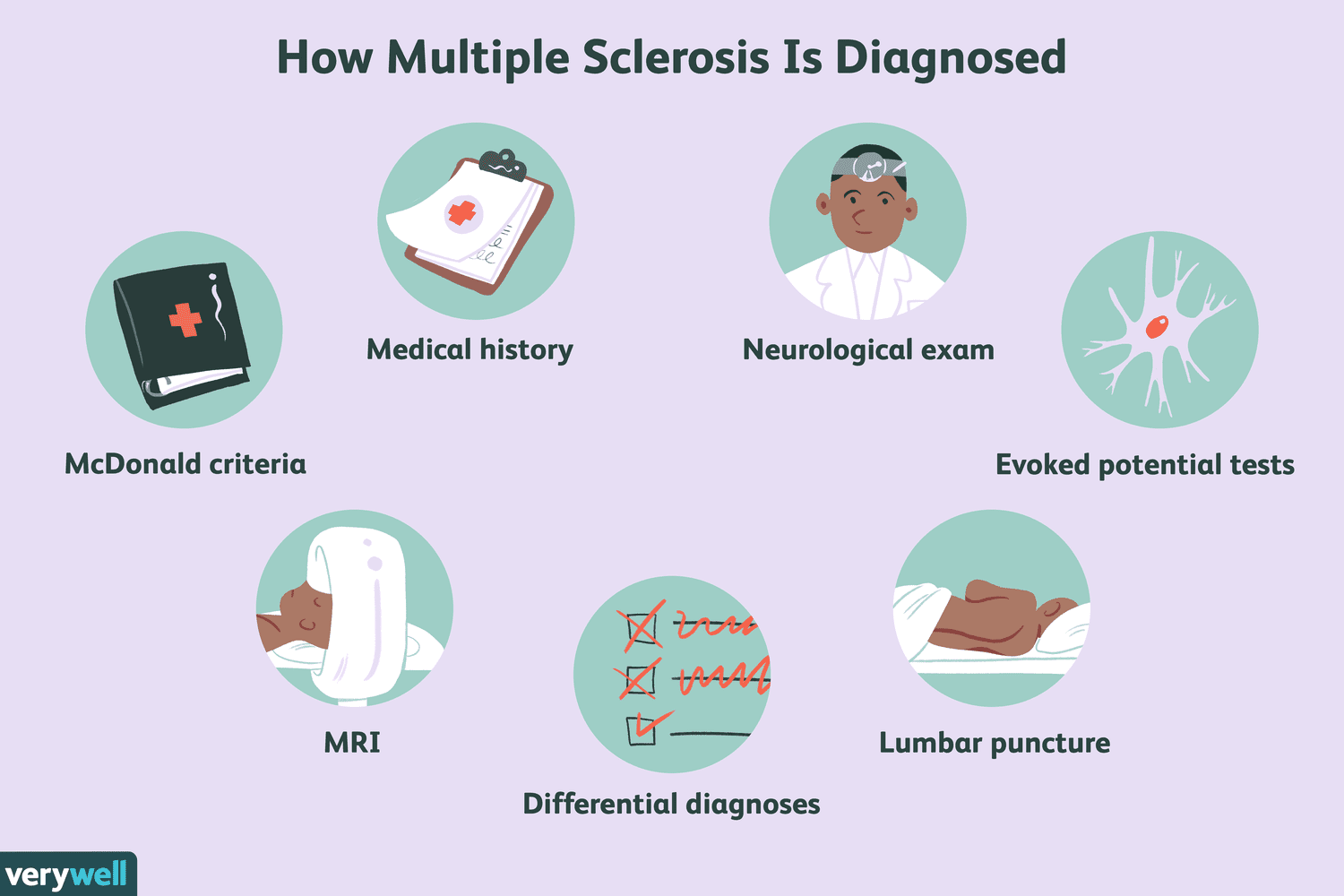
How is MS diagnosed?
Pathognomonic tests do not exist to diagnose multiple sclerosis. Diagnosis is established by considering the patient's history and physical examination, along with MRI findings, evoked potentials, and cerebrospinal fluid (CSF) or blood studies, while also excluding other causes of the patient's symptoms. Clinically, a diagnosis of multiple sclerosis is supported by evidence of one or more relapses, which can be confirmed through objective clinical evidence of one or more lesions or objective clinical evidence of one lesion with reliable historical evidence of a prior relapse.
Dissemination in space (DIS) and dissemination in time (DIT) are 2 key criteria for accurately diagnosing multiple sclerosis. DIS is assessed by integrating information from the patient's history and physical examination to determine the location of CNS involvement. MRI and evoked potentials also have vital roles in establishing DIS. DIT is established by charting the disease course with a thorough history and documenting the presence of multiple exacerbations over time. The 2010 McDonald criteria determined that new lesions can demonstrate DIT on a follow-up MRI compared to a baseline scan.
DIS is established by observing at least a T2 lesion in 2 of the 4 following CNS sites—spinal cord, infratentorial, juxtacortical, and periventricular regions. Revisions in the 2017 McDonald criteria increased the sensitivity of diagnosis by introducing oligoclonal bands in the CSF analysis as a marker for establishing DIT. Symptomatic lesions were also included to establish DIT and DIS, and cortical lesions were used to demonstrate DIS.
Evoked potentials help demonstrate slowed conduction indicative of subclinical involvement. These findings are often asymmetric. MRI, CSF, and blood studies are essential in ruling out other aetiologies. When possible, all patients should undergo an MRI. Additionally, specific blood studies such as complete blood count (CBC), thyroid-stimulating hormone (TSH), vitamin B12 levels, erythrocyte sedimentation rate (ESR), and antinuclear antibody (ANA) testing should be performed as part of the diagnostic workup.
