Lower back pain affects 60-85% of adults during some point in their lives (Anderson et al 1999). About 90% of those recover within 6 weeks with mild and transient symptoms (Dillane J et al 1966). In United States, incidence of low back pain is 3% in 20-29 aged people and it rises to >80% in 40 years or over population.
The term Spondylosis has been utilized in literature in many different contexts such as arthrosis, spondylitis, osteoarthritis and hypertrophic arthritis (Middleton & Fish 2009). Lumbar spondylosis is a term that may be applied to any degenerative conditions affecting the disks, vertebral bodies and joints of the Lumbar spine (Schneck et al 1985) (Gibson et al 2005).
Pathogenesis
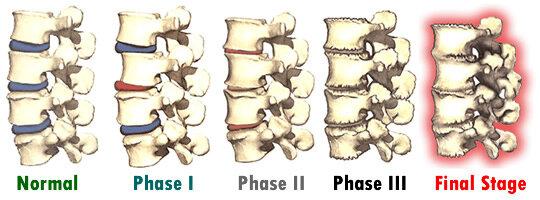
Kirkaldy Willis and Bernad believed that the intervertebral disks undergo a “degenerative cascade” of three overlapping phases that may occur over the course of several years.
These pathophysiological changes can clinically present with symptoms such as uni or bilateral lower back pain which can be localized or widespread in the lumbo-pelvic region. Pain can also refer in the buttocks, hips, lower extremities depending on the spinal nerve involvement. Nociception generating receptors have been identified in intervertebral disks, facet and Sacro-iliac joints, nerve root dura and myofascial structures.
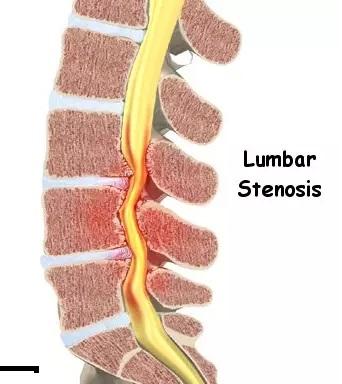
The degeneration of anatomical structures in the spine such as osteophytic growth, thickening of ligamentum flavum or bulging discs may lead to narrowing of the spinal foramen resulting in Spinal Canal Stenosis.
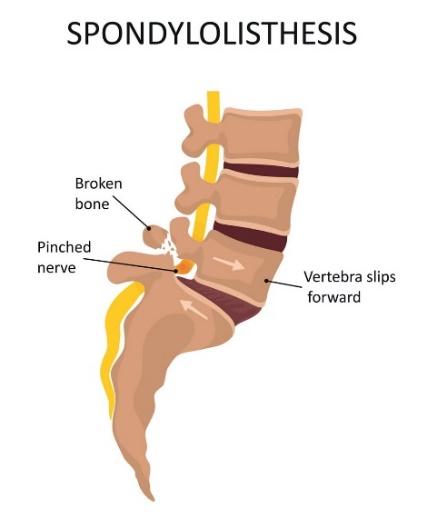
Facet joint and disk degeneration can lead to instability and forward movement of one vertebra over another. This can result in causing varied degree of ligamentum flavum strain and slipping of vertebra, fracturing the pars interarticularis resulting into Spondylolisthesis.
Lumbar radiculopathy is often found along with the group of symptoms as a result of the extensive intervertebral disk space reduction resulting in nerve root compression. It can cause motor weakness and sensory impairments in lower extremities. In advanced cases of lumbar spondylosis, it is very important to monitor symptoms and educate patients to make them aware of red flags such as Cauda equina Syndrome. In progressive degeneration, the degree of spinal canal stenosis can lead to debilitating impairments of sensory-motor functions of lower extremities, balance and gait, bowel and bladder control and sexual functions.
Diagnosis
Clinical testing such as examination of range of movements, accessory movement tests and basic palpatory examination of Lumbar region is essential to form clinical reasoning and basis to include special tests.
Special tests such as Straight leg raise, FABER`s, Quadrant, Stork, neurodynamic tests for the peripheral nerves, etc. can point to specific structures that may be involved in the Lumbar spondylosis. Based on severity of symptoms and clinical testing results, imaging can be recommended. An X-ray, CT or MRI can provide further insight into degree of pathophysiology specially where invasive intervention is under consideration and/or to rule out red flags of the spinal column like
Outcome measures
Patient can be given a numeric rating scale to check pain scores ranging from 0 (no pain) to 10 (worst imaginable pain).
Oswestry Disability Index can be given to the patient to rate percentage of disability due to low back pain in activities of daily living.
Patient specific functional score can be used to rate functional activities subjectively from 0 (unable to perform) to 10 (no limitation to perform the activity).
Role of physical therapy
The World Health Organization (WHO) estimated that in 2020, lower back pain affected 619 million globally, which is projected to increase to 843 million by 2050. Lower back pain has the highest prevalence globally among musculoskeletal conditions and is the leading cause of disability and economic burden worldwide.
The WHO broadly categorizes lower back pain (LBP) into specific and non-specific LBP (https://www.who.int/news-room/fact-sheets/detail/low-back-pain). Specific low back pain is caused by a certain disease or structural problem in the spine, or when pain radiates from another part of the body.
Non-specific LBP is when it isn`t possible to identify a specific disease or structural reason to explain the pain. Non-specific LBP amounts to nearly 90% of all the LBP cases. WHO emphasizes the role of physical therapy, psychological and social support, reducing strain-causing injuries and lifestyle changes as fundamentals in management of LBP.
Lumbar Spondylosis appears to be an age-related condition (Buckwalter 2004) which has no proven correlation with lifestyle, height, weight, addictions or physical activity (Yoshimura et al 2000). Adiposity is seen as risk factor in British, but not Japanese population.
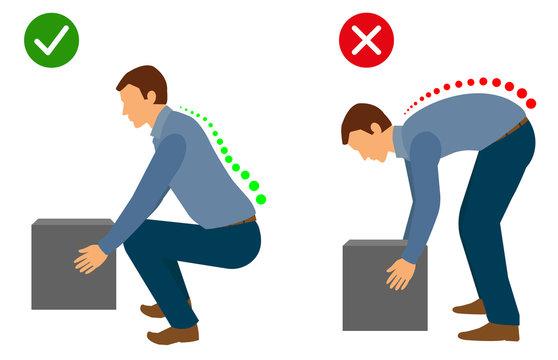
Several studies support the role of ergonomics and physical therapy in the management of low back pain and degenerative conditions of Lumbar spine. For example, using the appropriate body postures while lifting a heavy weight from floor.
For desk workers who spend hours in sustained seated postures, it is important to have the right biomechanics to prevent sustained over-loading and over-straining of the spinal structures.

Exercise therapy remains one of the conservative mainstays of treatment for chronic lumbar spine pain, and maybe tailored to include aerobic exercises, muscle strengthening and stretching exercises (Hayden et al 2005). According to Vibert et al 2006, most physicians begin with a 1–2-day period of rest followed by a short course of anti-inflammatory medication after ruling out gastrointestinal contraindications.
Core abdominal muscle training for 10 weeks resulted in reduced pain intensity and functional disability that was maintained at 30-week follow up (O`Sullivan 1996). Lindgren et al (1993) found that exercise therapy in patients with chronic LBP and segmental instability can improve strength and electromyographic parameters of para-spinal muscles but not radiographic findings. Similar study (Hayden et al 2005) proves the use of aerobic training, stretching and strengthening exercises to reduce chronic low back pain and reduce disability. As muscle imbalance has been associated with inaccurate posture and functional disability (Nava-Bringas 2014) (Kreiner et al 2016), the aim of physical therapy should be achieving trunk muscle balance rather than muscle strength alone.
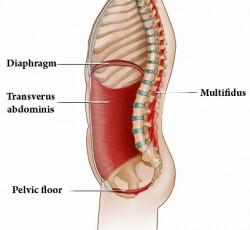
Weakness of muscles around lumbar region has been shown to contribute to segmental instability and low back pain even in absence of structural defects (Delitto et al 2012). The core is a box structure made of the abdominal muscles at the front and sides, para-spinal and gluteal muscles at the back, diaphragm at the roof and pelvic/hip girdle as the base (Akuthota et al 2004).
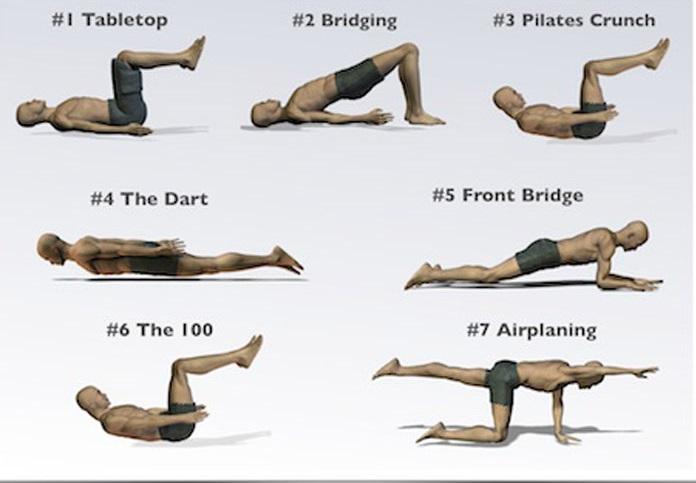
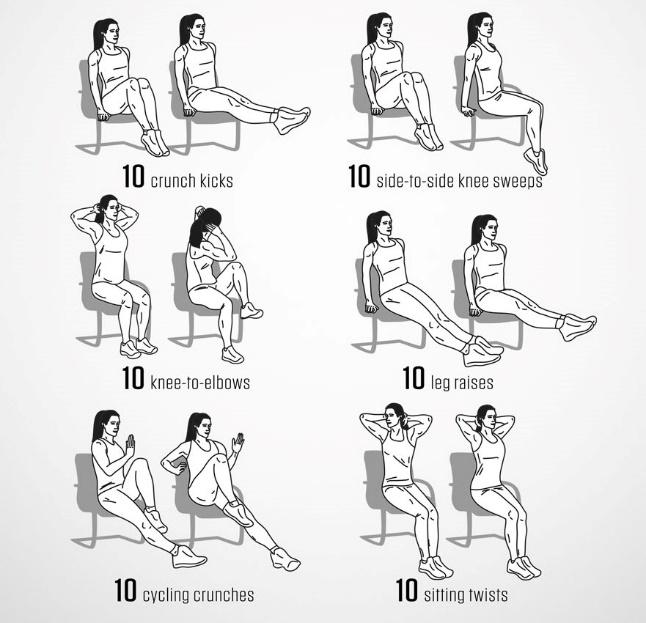
Core muscle training must be performed in lying, sitting and standing positions. Few examples of basic core stabilization exercises in various positions are as follows –

Spinal Joint mobilizations can be considered as an adjunct to achieve pain relief and mobility in pain/stiffness dominant cases after assessing patient suitability. The therapist evaluates tissue irritability prior to administering joint mobilization technique. Pharmacotherapy serves as an adjunct, if not primary treatment method to achieve pain relief, minimize swelling, disability and improve quality of life. There is weak evidence that advocates the use of bracing, therapeutic ultrasound, electrical stimulation and activity modification (Pettine et al 1993, Fellander-Tsai et al 1998).
There is emerging evidence in the area of pain neuroscience supporting role of education and awareness of patient`s condition (low back pain) and the potential sources of pain. It has been proved that by making them learn the role of brain in pain modulation, they are able to manage their condition better and have a better quality of life (Oosterwijck et al 2011) (Louw et al 2019)
If conservative therapies are not beneficial as expected, invasive methods such as Injection therapy, nerve block or surgery are considered.
