What are the acute complications of Diabetes?
What are the long-term complications for diabetes?
Blood glucose levels that remain high for too long can damage your body’s tissues and organs. This is mainly due to damage to your blood vessels and nerves, which support your body’s tissues.
Cardiovascular (heart and blood vessel) issues are the most common type of long-term diabetes complication. They include:
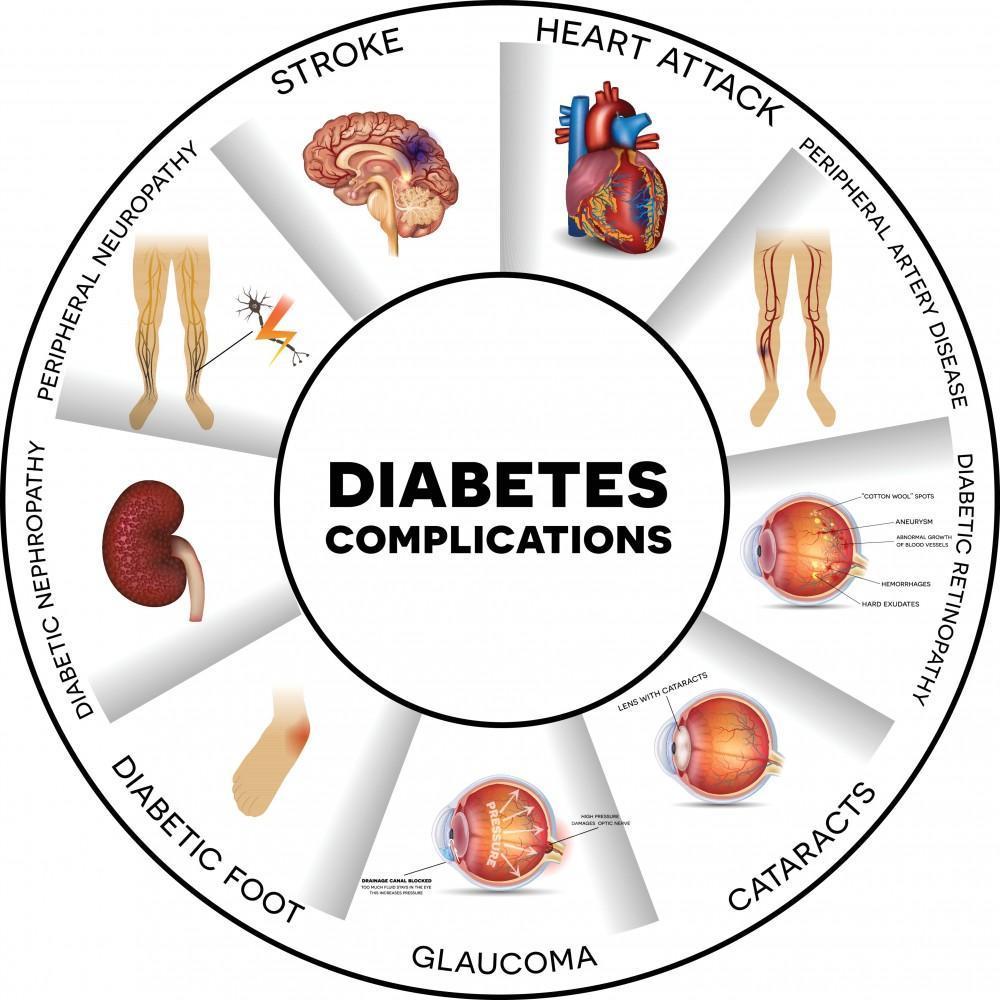
Other diabetes complications include:
Living with diabetes can also affect your mental health. People with diabetes are two to three times more likely to have depression than people without diabetes. (https://my.clevelandclinic.org/health/diseases/7104-diabetes)
How is diabetes diagnosed?
Type 1 diabetes symptoms often start suddenly and are often the reason for checking blood sugar levels. Because symptoms of other types of diabetes and prediabetes come on more gradually or may not be easy to see, the American Diabetes Association (ADA) has developed screening guidelines. The ADA recommends that the following people be screened for diabetes:
Tests for type 1, type 2 and prediabetes:
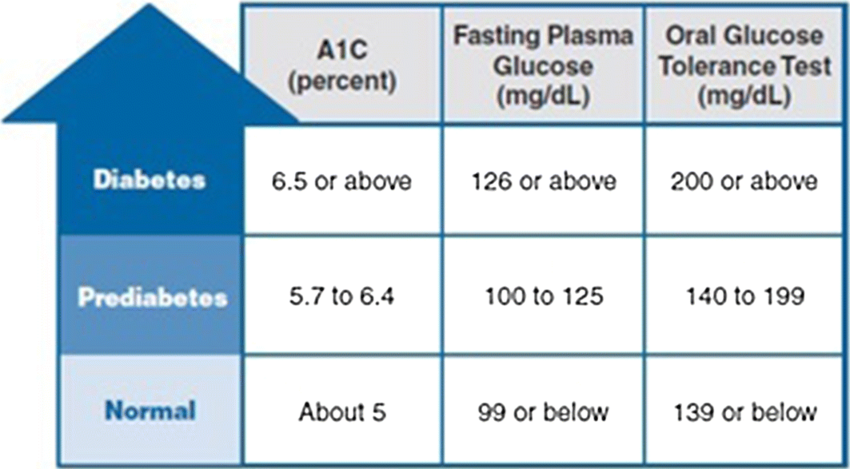
Fasting blood sugar test - A fasting blood sugar level less than 100 mg/dL (5.6 mmol/L) is normal. A fasting blood sugar level from 100 to 125 mg/dL (5.6 to 6.9 mmol/L) is considered prediabetes. If it's 126 mg/dL (7 mmol/L) or higher on two separate tests, you have diabetes.

A blood sugar level less than 140 mg/dL (7.8 mmol/L) is normal. A reading of more than 200 mg/dL (11.1 mmol/L) after two hours means you have diabetes. A reading between 140 and 199 mg/dL (7.8 mmol/L and 11.0 mmol/L) means you have prediabetes.
If your provider thinks you may have type 1 diabetes, they may test your urine to look for the presence of ketones. Ketones are a byproduct produced when muscle and fat are used for energy. Your provider will also probably run a test to see if you have the destructive immune system cells associated with type 1 diabetes called autoantibodies.
Your provider will likely see if you're at high risk for gestational diabetes early in your pregnancy. If you're at high risk, your provider may test for diabetes at your first prenatal visit. If you're at average risk, you'll probably be screened sometime during your second trimester. (https://www.mayoclinic.org/diseases-conditions/diabetes/diagnosis-treatment/drc-20371451)
What is the treatment for diabetes?
The physiology and treatment of diabetes are complex and require a multitude of interventions for successful disease management. Diabetic education and patient engagement are critical in management. Patients have better outcomes if they can manage their diet (carbohydrate and overall caloric restriction), exercise regularly (more than 150 minutes weekly), and independently monitor glucose. Lifelong treatment is often necessary to prevent unwanted complications. Ideally, glucose levels should be maintained at 90 to 130 mg/dL and HbA1c at less than 7%. While glucose control is critical, excessively aggressive management may lead to hypoglycaemia, which can have adverse or fatal outcomes.
Since T1DM is a disease primarily due to the absence of insulin, daily administration of insulin injections, or an insulin pump, is the mainstay of treatment.
In T2DM, diet and exercise may be adequate treatments, especially initially. Other therapies may target insulin sensitivity or increase insulin secretion by the pancreas. The specific subclasses for drugs include biguanides (metformin), sulfonylureas, meglitinides, alpha-glucosidase inhibitors, thiazolidinediones, glucagonlike-peptide-1 agonist, dipeptidyl peptidase IV inhibitors (DPP-4), selective, amylinomimetics, and sodium-glucose transporter-2 (SGLT-2) inhibitors. Metformin is the first line of the prescribed diabetic medications and works by lowering basal and postprandial plasma glucose. Insulin administration may also be necessary for T2DM patients, especially those with inadequate glucose management in the advanced stages of the disease. In morbidly obese patients, bariatric surgery is a possible means to normalize glucose levels. It is recommended for individuals who have been unresponsive to other treatments and who have significant comorbidities.
Regular screenings are necessary since microvascular complications are a feared complication of diabetes. Regular diabetic retinal exams should be performed by qualified medical personnel to assess for diabetic retinopathy. Neurologic examination with monofilament testing can identify patients with neuropathy at risk for amputation. Clinicians can also recommend patients perform daily foot inspections to identify foot lesions that may go unnoticed due to neuropathy. Low-dose tricyclic antidepressants, duloxetine, anticonvulsants, topical capsaicin, and pain medications may be necessary to manage neuropathic pain in diabetes. The FDA has approved pregabalin and duloxetine for the treatment of diabetic peripheral neuropathy. Tricyclic antidepressants and anticonvulsants have also seen use in the management of the pain of diabetic neuropathy with variable success.

Urine microalbumin testing can also assess for early renal changes from diabetes with albuminuria greater than 30mg/g creatinine along with the estimated GFR. The antiproteinuric effect of the angiotensin-converting enzyme (ACE) inhibitors and the angiotensin receptor blockers (ARBs) makes them the preferred agents to delay the progression from microalbuminuria to macroalbuminuria in patients with both Type 1 or Type 2 diabetes mellitus.
The ADA also recommends regular blood pressure screening for diabetics, with the goal being 130 mmHg systolic blood pressure and 85 mmHg diastolic blood pressure. Pharmacologic therapy for hypertensive diabetics typically involves angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, diuretics, beta-blockers, and/or calcium channel blockers. The ADA recommends lipid monitoring for diabetics with a goal of low-density lipoprotein cholesterol (LDL-C) being less than 100 mg/dL if no cardiovascular disease (CVD) and less than 70 mg/dl if atherosclerotic cardiovascular disease (ASCVD) is present. Statins are the first-line treatment for the management of dyslipidaemia in diabetics. The ADA suggests that low dose aspirin may also be beneficial for diabetic patients who are at high risk for cardiovascular events; however, the role of aspirin in reducing cardiovascular events in patients with diabetes remains unclear. (https://www.ncbi.nlm.nih.gov/books/NBK551501/)
