
Cervical Spondylosis: Causes and Treatments
Cervical Spondylosis is often referred to as the arthritis of the neck, which includes general wear and tear that affects the cervical spine. “Cervical” refers to the seven stacked vertebral bones in the neck region. “Spondylosis” is when parts of the spine begin to wear out which is often age-related. The condition is also commonly known as “osteoarthritis” of the neck.
Cervical spondylosis (CS) is a natural consequence of aging and often appears when people are in their 30s. By 60, nine out of ten people are expected to show degenerative changes in the cervical spine. (https://my.clevelandclinic.org/health/diseases/17685-cervical-spondylosis)
What is the etiology of CS?
The primary risk factor and contributor to the incidence of CS is age-related degeneration of the intervertebral disc and cervical spine elements. Degenerative changes in surrounding structures including the uncovertebral joints, facet joints, posterior longitudinal ligaments (PLL) and ligamentum flavum all combine towards narrowing of the spinal canal and intervertebral foramina. Consequently, the spinal cord, spinal vasculature and nerve roots can be compressed resulting in the 3 clinical syndromes of cervical spondylosis: axial neck pain, cervical myelopathy and cervical radiculopathy.
Factors that can contribute to an accelerated disease process and early-onset cervical spondylosis include exposure to significant spinal trauma, a congenitally narrow vertebral canal, dystonic cerebral palsy affecting cervical spine musculature manual labor and specific high impact athletic activities like rugby or horse-back riding. (https://www.ncbi.nlm.nih.gov/books/NBK551557/)
What is the pathophysiology of CS?
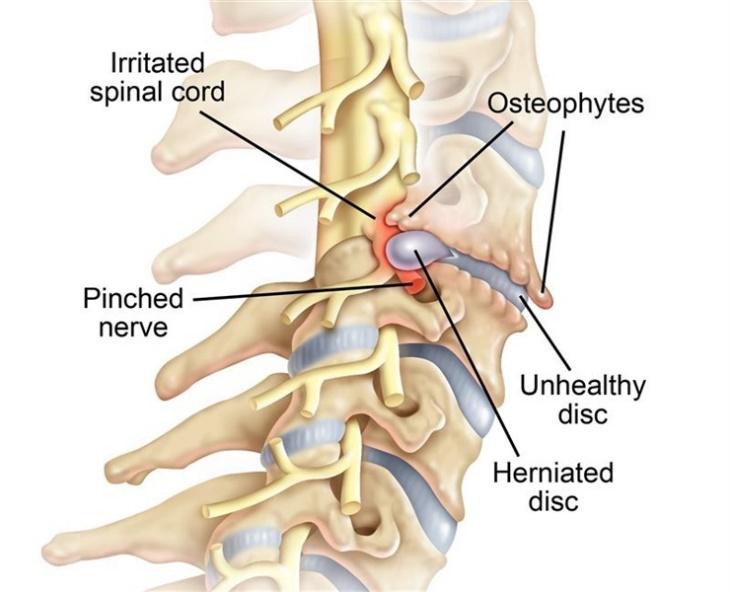
The pathogenesis of cervical spondylosis involves a degenerative cascade that produces biomechanical changes in the cervical spine, manifesting as secondary compression of neural and vascular structures. An increase in the keratin-chondroitin ratio prompts changes to the proteoglycan matrix resulting in loss of water, protein, and mucopolysaccharides within the intervertebral disc. Desiccation of the disc causes the nucleus pulposus to lose its elasticity as it shrinks and becomes more fibrous. As the nucleus pulposus loses its ability to maintain weight-bearing loads effectively, it begins to herniate through the fibres of the annulus fibrosus and contributes to the loss of disc height, ligamentous laxity, and buckling, and compression of the cervical spine. With further disc desiccation, the annular fibres become more mechanically compromised under compressive loads, producing significant alterations in the load distribution along the cervical spine. The result is a reversal of the normal cervical lordosis. Progression of the kyphosis causes the annular and Sharpey’s fibres to peel off from the vertebral body edges, resulting in reactive bone formation. These bone spurs or osteophytes can form along the ventral or dorsal margins of the cervical spine, which can then project into the spinal canal and intervertebral foramina. Furthermore, disruption in the load balance along the spinal column generates greater axial loads onto the uncovertebral and facet joints which triggers hypertrophy or enlargement of the joints and accelerates bony spur formation into the surrounding neural foramen. These degenerative changes lead to loss of cervical lordosis and movement, as well as a reduction in the spinal canal diameter. (https://www.ncbi.nlm.nih.gov/books/NBK551557/)
What are the symptoms of CS?
- Neck pain and stiffness which is worse particularly in the morning.
- A bump or knot around your neck related to muscle tension and spasm.
- Clicking, popping or grinding sound while moving the neck.
- Dizziness
- Cervicogenic headaches
- Limited neck range of movements
- Pain may radiate in scapula or upper extremities with associated tingling ad numbness.
- In advanced stages there may be muscle weakness in upper extremities (https://my.clevelandclinic.org/health/diseases/17685-cervical-spondylosis)
How is CS diagnosed?
- Patient presents with neck pain and stiffness that is most severe in upright position and gets aggravated with loading of the spine or extreme range of neck movements.
- Tender “trigger” points are frequently present within upper trapezius, cervical paraspinals and peri-scapular muscles.
- Electric shock-like sensations radiating down the spine and into the extremities with cervical flexion is a positive Lhermitte`s sign, which is concerning for cervical spondylotic myelopathy (CSM). A more specific sign for CSM is Hoffman`s sign which is elicited by flicking the patient`s distal phalanx of the middle finger and observing reflexive flexion of the thumb and/or index finger.
- All physical exams should include a meticulous evaluation of bilateral extremities for muscle strength, sensation, and deep tendon reflexes in order to look for weakness in a myotome distribution, sensory deficits in a dermatomal pattern, and reflex changes, respectively; all of which can help to identify the compromised nerve root(s) and/or myelopathy.
- Additional neurological testing should include gait and balance tests, coordination test, Romberg`s test for examining dorsal column integrity. (https://www.ncbi.nlm.nih.gov/books/NBK551557/)
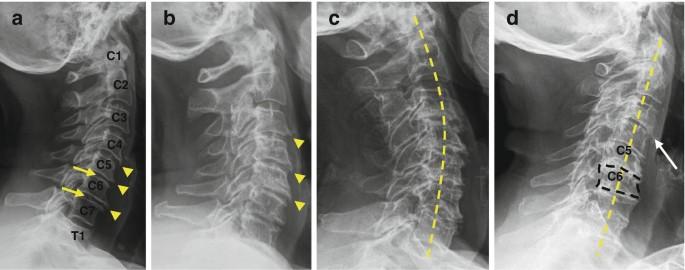
- CS can be graded using a very old but reliable classification devised by Jonas Kellgren. It is based on findings on a lateral cervical spine radiograph although it can also be applied to MRI evaluation of spine.
If there is radiating pain down the upper limb with head extension and ipsilateral head rotation to the affected side, then it’s considered a positive Spurling`s test for cervical radiculopathy. In some cases, manual neck distraction might alleviate radicular pain.
The key parameters are osteophyte formation, intervertebral disc height narrowing and vertebral end-plate sclerosis.
- grade 0 (normal)
- no degenerative changes
- grade 1 (minimal/early)
- minimal anterior osteophyte formation
- no reduction of intervertebral disc height
- no vertebral endplate sclerosis
- grade 2 (mild)
- definite anterior osteophyte formation
- subtle or no reduction in intervertebral disc height (<25%)
- just recognisable sclerosis of the endplates
- grade 3 (moderate)
- definite anterior osteophyte formation
- moderate narrowing of the disc space (25-75%)
- definite sclerosis of the endplates and osteophyte sclerosis
- grade 4 (gross)
- large and multiple large osteophyte formation is seen
- severe narrowing of the disc space (>75%)
- sclerosis of the endplates with irregularities (https://radiopaedia.org/articles/cervical-degenerative-spondylosis-grading-1)
How will imaging help?
- Cervical spine X-ray can show reduce disk space, bone spurs and osteophytes indicative of degeneration. They can often help rule out fractures, tumours, cancers and infection.
- Magnetic resonance imaging can produce detailed images that can help identify source of radicular symptoms and area of nerve root compression. A CT scan also helps to identify the details of pathophysiological changes in CS.
- Electromyography helps to identify neuromuscular involvement in cases where there in nerve root compression.
- Nerve conduction testing also helps to point at type of degeneration in case of root compression at the intervertebral foramen. (https://www.healthline.com/health/cervical-spondylosis#treatment)
How is CS treated?
Choice of treatment depends on severity of patient`s symptoms. In the absence of red flags and significant myelopathy, the goals of treatment are to relieve pain, improve functional mobility and participation id daily activities. Non-operative management includes:
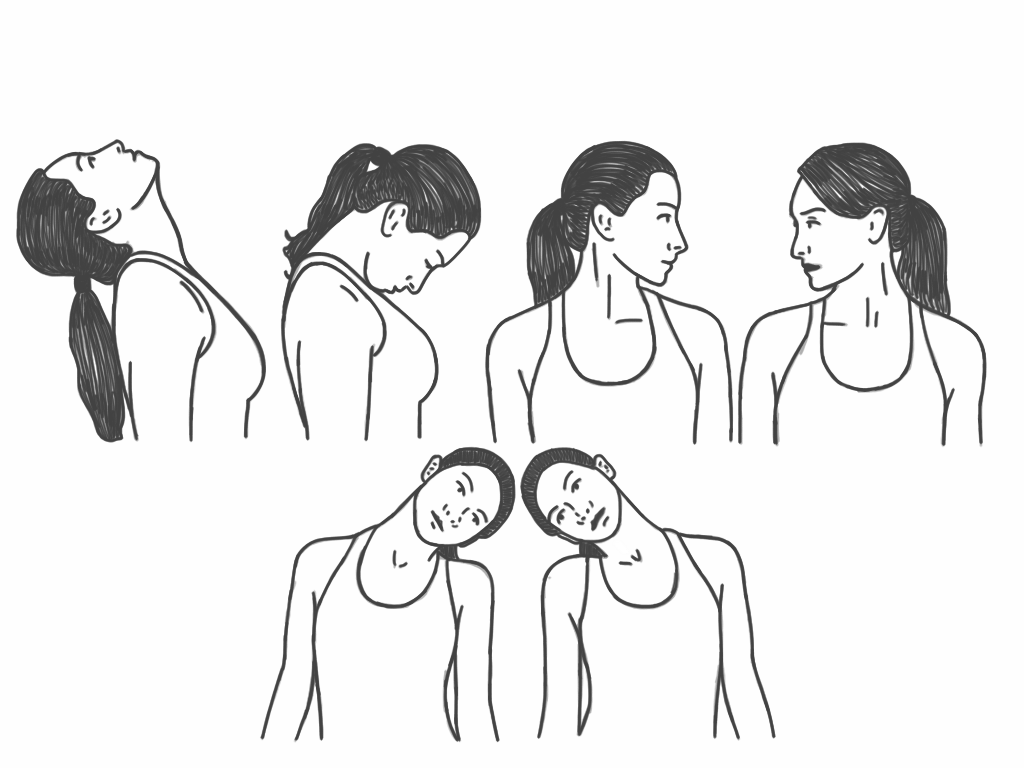
- Physical therapy – includes basic mobility and isometric strengthening of neck and upper back muscles for 6 weeks. Modalities such as heat, cold, therapeutic ultrasound, TENS lack sufficient evidence regarding their efficacy in treating acute or chronic neck pain. However, in patients experiencing radicular pain, cervical traction may be incorporated to alleviate the nerve root compression that occurs with foraminal stenosis.
- Pain relief can be provided with the help of NSAIDs such as ibuprofen, short course of corticosteroid such as prednisone in case of severe pain and muscle relaxants such as cyclobenzaprine in cases of severe muscle spasm. (https://www.mayoclinic.org/diseases-conditions/cervical-spondylosis/diagnosis-treatment/drc-20370792)
- Surgery is typically indicated in progressive cervical myelopathy and in those who have tried conservative therapy with not much symptom relief. The surgical approach depends on the clinical syndrome and the site of pathology.
- In patients who experience radicular pain due to central or bilateral herniation, an anterior approach is preferable. Whereas either an anterior or posterior approach is an option for lateral disc lesion. (https://www.ncbi.nlm.nih.gov/books/NBK551557/)
Few studies have shown symptom reduction with use of trigger point injection over myofascial trigger points. A systematic review done in 2019 show patient having significant pain relief following epidural steroid injection. Long-term pain relief was also seen in a systematic review done in 2015 to study effects of radiofrequency lesioning, medial branch block and facet joint injection in CS cases.
